短暂性左束支传导阻滞伴极高冠状动脉钙:一例报告。
IF 2.2
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 1
摘要
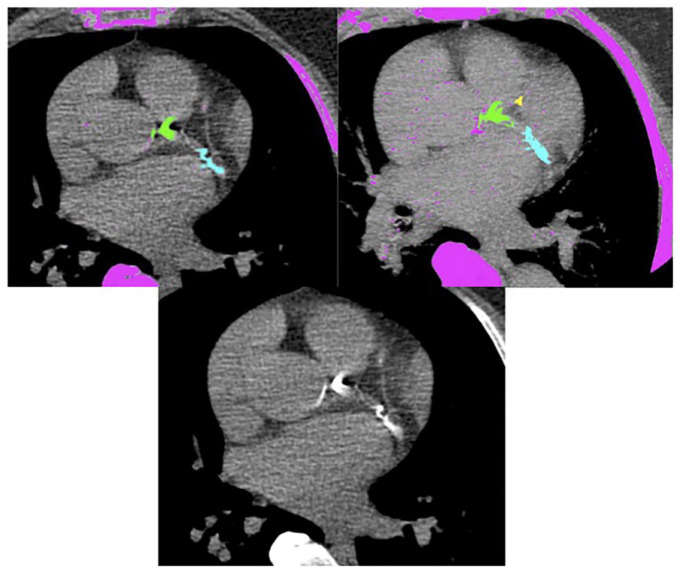
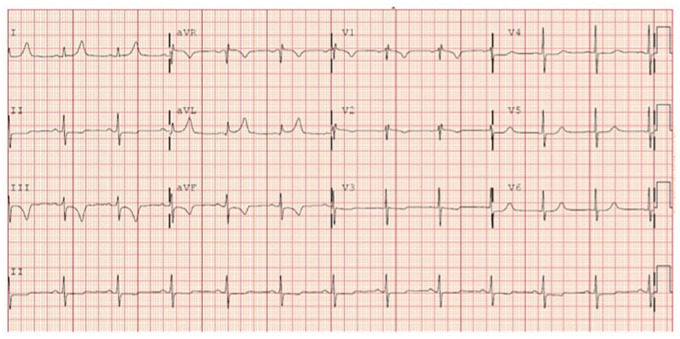
冠状动脉钙(CAC)是亚临床冠状动脉动脉粥样硬化的指标,与动脉粥样硬化性心血管疾病(ASCVD)风险密切相关。然而,CAC在住院患者中很少报道,以指导胸痛管理。我们报告了一例64岁女性的CAC非常高,她患有高血压、2型糖尿病和高脂血症,并伴有呼吸困难。初始心电图(ECG)显示传导正常,心率为76次/分,但V1-V4出现新的T波倒置,高敏肌钙蛋白I(hsTnI)值为6 ng/L(正常本文章由计算机程序翻译,如有差异,请以英文原文为准。
Transient left bundle branch block associated with very high coronary artery calcium: a case report.
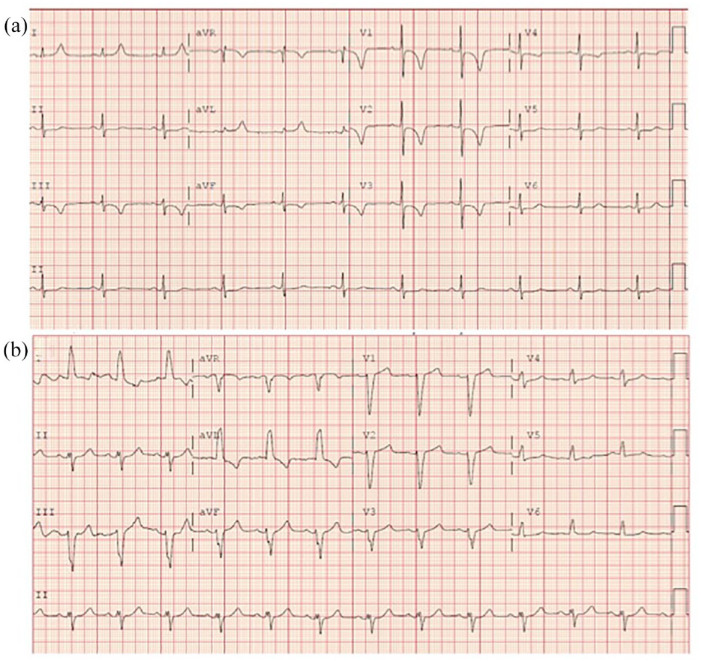
Coronary artery calcium (CAC) is the measure of subclinical coronary artery atherosclerosis most strongly associated with atherosclerotic cardiovascular disease (ASCVD) risk. However, CAC is rarely reported in the inpatient setting to guide chest pain management. We present a case of very high CAC in a 64-year-old woman with hypertension, type 2 diabetes, and hyperlipidemia presenting with dyspnea. Initial electrocardiogram (ECG) demonstrated normal conduction with a heart rate of 76 beats/min, but new T-wave inversions in V1–V4 and a high-sensitivity troponin-I (hsTnI) value of 6 ng/L (normal < 6 ng/L). Repeat ECG in the emergency department showed normal sinus rhythm (heart rate of 80 beats/min); however, it subsequently demonstrated a left bundle branch block (LBBB) with a repeat hsTnI of 7 ng/L. Stress testing with pharmacologic single-photon emission computerized tomography did not show scintigraphic evidence of ischemia but noted extensive CAC and a concern for balanced ischemia. Subsequent coronary computed tomography angiography (CCTA) showed nonobstructive disease and a total Agatston CAC score of 1262. Invasive evaluation with left heart catheterization was deferred given the patient’s unchanged symptoms and CCTA findings. Statin therapy was intensified and aspirin, metoprolol succinate, and antihypertension therapies were continued. Initiation of glucose-lowering therapy and lipoprotein(a) testing was strongly recommended on follow-up. Our case suggests that CAC ⩾ 1000 may be incidentally associated with transient LBBB during the workup of coronary artery disease. Here, we specifically show that functional testing that incorporates measurement of CAC burden can help to improve ASCVD-preventive pharmacotherapy initiation and intensification beyond the identification of obstructive disease alone.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Therapeutic Advances in Cardiovascular Disease
CARDIAC & CARDIOVASCULAR SYSTEMS-
CiteScore
3.50
自引率
0.00%
发文量
11
审稿时长
9 weeks
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


