{"title":"一名14岁男孩因阿莫西林引起严重多形性红斑。","authors":"Mami Kurihara, Shingo Yamanishi, Saeko Ozaki, Ruby Pawankar","doi":"10.5415/apallergy.0000000000000108","DOIUrl":null,"url":null,"abstract":"<p><p>The most common cause of erythema multiforme (EM) in children is infectious diseases which account for approximately 90% of cases. Drug eruptions are another common cause. Here we are reporting about a male patient aged 14 years with lymphadenitis who developed severe diffuse erythema during the course of treatment with medications including several antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs). Based on the pathological findings of the skin biopsy, the skin rash was due to EM. Upon investigating the underlying cause of EM, viral antibody was positive for Coxsackie A6, lymphocyte transformation testing (LTT) was positive for one of the NSAIDs, and the patch test (PT) was positive for amoxicillin. Based on the pattern of distribution of the skin rash, the cause of EM was considered to be drug-induced eruption due to amoxicillin. In this case, we did not derive a diagnosis of drug eruption without investigating the possibility of drug induction, because most cases of EM in children are induced by infection and the antibody against Coxsackie A6 was elevated. To diagnose the possibility of amoxicillin-induced EM, it was important to distinguish between the distribution patterns of infectious versus drug-induced EM and to evaluate the possibility of drug induction by both LTT and PT. If the diagnosis of amoxicillin-induced EM, had not been made, the potential recurrence of EM with amoxicillin could have occurred.</p>","PeriodicalId":8488,"journal":{"name":"Asia Pacific Allergy","volume":"13 3","pages":"135-138"},"PeriodicalIF":2.1000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/45/cf/pa9-13-135.PMC10516312.pdf","citationCount":"0","resultStr":"{\"title\":\"A 14-year-old boy with severe erythema multiforme due to amoxicillin.\",\"authors\":\"Mami Kurihara, Shingo Yamanishi, Saeko Ozaki, Ruby Pawankar\",\"doi\":\"10.5415/apallergy.0000000000000108\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The most common cause of erythema multiforme (EM) in children is infectious diseases which account for approximately 90% of cases. Drug eruptions are another common cause. Here we are reporting about a male patient aged 14 years with lymphadenitis who developed severe diffuse erythema during the course of treatment with medications including several antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs). Based on the pathological findings of the skin biopsy, the skin rash was due to EM. Upon investigating the underlying cause of EM, viral antibody was positive for Coxsackie A6, lymphocyte transformation testing (LTT) was positive for one of the NSAIDs, and the patch test (PT) was positive for amoxicillin. Based on the pattern of distribution of the skin rash, the cause of EM was considered to be drug-induced eruption due to amoxicillin. In this case, we did not derive a diagnosis of drug eruption without investigating the possibility of drug induction, because most cases of EM in children are induced by infection and the antibody against Coxsackie A6 was elevated. To diagnose the possibility of amoxicillin-induced EM, it was important to distinguish between the distribution patterns of infectious versus drug-induced EM and to evaluate the possibility of drug induction by both LTT and PT. If the diagnosis of amoxicillin-induced EM, had not been made, the potential recurrence of EM with amoxicillin could have occurred.</p>\",\"PeriodicalId\":8488,\"journal\":{\"name\":\"Asia Pacific Allergy\",\"volume\":\"13 3\",\"pages\":\"135-138\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/45/cf/pa9-13-135.PMC10516312.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asia Pacific Allergy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5415/apallergy.0000000000000108\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asia Pacific Allergy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5415/apallergy.0000000000000108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ALLERGY","Score":null,"Total":0}
A 14-year-old boy with severe erythema multiforme due to amoxicillin.
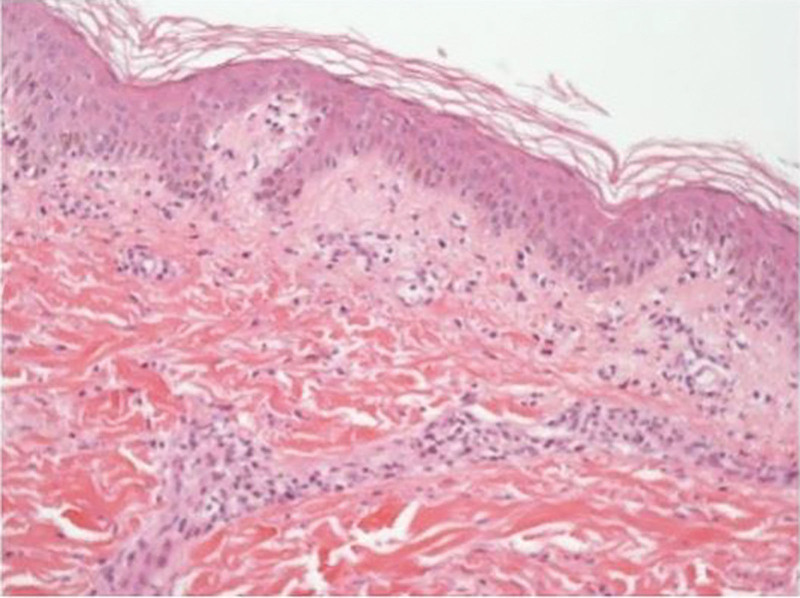
The most common cause of erythema multiforme (EM) in children is infectious diseases which account for approximately 90% of cases. Drug eruptions are another common cause. Here we are reporting about a male patient aged 14 years with lymphadenitis who developed severe diffuse erythema during the course of treatment with medications including several antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs). Based on the pathological findings of the skin biopsy, the skin rash was due to EM. Upon investigating the underlying cause of EM, viral antibody was positive for Coxsackie A6, lymphocyte transformation testing (LTT) was positive for one of the NSAIDs, and the patch test (PT) was positive for amoxicillin. Based on the pattern of distribution of the skin rash, the cause of EM was considered to be drug-induced eruption due to amoxicillin. In this case, we did not derive a diagnosis of drug eruption without investigating the possibility of drug induction, because most cases of EM in children are induced by infection and the antibody against Coxsackie A6 was elevated. To diagnose the possibility of amoxicillin-induced EM, it was important to distinguish between the distribution patterns of infectious versus drug-induced EM and to evaluate the possibility of drug induction by both LTT and PT. If the diagnosis of amoxicillin-induced EM, had not been made, the potential recurrence of EM with amoxicillin could have occurred.
期刊介绍:
Asia Pacific Allergy (AP Allergy) is the official journal of the Asia Pacific Association of Allergy, Asthma and Clinical Immunology (APAAACI). Although the primary aim of the journal is to promote communication between Asia Pacific scientists who are interested in allergy, asthma, and clinical immunology including immunodeficiency, the journal is intended to be available worldwide. To enable scientists and clinicians from emerging societies appreciate the scope and intent of the journal, early issues will contain more educational review material. For better communication and understanding, it will include rational concepts related to the diagnosis and management of asthma and other immunological conditions. Over time, the journal will increase the number of original research papers to become the foremost citation journal for allergy and clinical immunology information of the Asia Pacific in the future.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


