Brijesh Patel, Scott A Chapman, Jake T Neumann, Aayush Visaria, Oluwabunmi Ogungbe, Sijin Wen, Maryam Khodaverdi, Priyal Makwana, Jasvinder A Singh, George Sokos
{"title":"患有严重急性呼吸系统综合征冠状病毒2型活动性癌症和已有心血管疾病的患者的结果。","authors":"Brijesh Patel, Scott A Chapman, Jake T Neumann, Aayush Visaria, Oluwabunmi Ogungbe, Sijin Wen, Maryam Khodaverdi, Priyal Makwana, Jasvinder A Singh, George Sokos","doi":"10.1186/s40959-023-00187-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To determine the impact of acute SARS-CoV-2 infection on patient with concomitant active cancer and CVD.</p><p><strong>Methods: </strong>The researchers extracted and analyzed data from the National COVID Cohort Collaborative (N3C) database between January 1, 2020, and July 22, 2022. They included only patients with acute SARS-CoV-2 infection, defined as a positive test by PCR 21 days before and 5 days after the day of index hospitalization. Active cancers were defined as last cancer drug administered within 30 days of index admission. The \"Cardioonc\" group consisted of patients with CVD and active cancers. The cohort was divided into four groups: (1) CVD (-), (2) CVD ( +), (3) Cardioonc (-), and (4) Cardioonc ( +), where (-) or ( +) denotes acute SARS-CoV-2 infection status. The primary outcome of the study was major adverse cardiovascular events (MACE), including acute stroke, acute heart failure, myocardial infarction, or all-cause mortality. The researchers analyzed the outcomes by different phases of the pandemic and performed competing-risk analysis for other MACE components and death as a competing event.</p><p><strong>Results: </strong>The study analyzed 418,306 patients, of which 74%, 10%, 15.7%, and 0.3% had CVD (-), CVD ( +), Cardioonc (-), and Cardioonc ( +), respectively. The Cardioonc ( +) group had the highest MACE events in all four phases of the pandemic. Compared to CVD (-), the Cardioonc ( +) group had an odds ratio of 1.66 for MACE. However, during the Omicron era, there was a statistically significant increased risk for MACE in the Cardioonc ( +) group compared to CVD (-). Competing risk analysis showed that all-cause mortality was significantly higher in the Cardioonc ( +) group and limited other MACE events from occurring. When the researchers identified specific cancer types, patients with colon cancer had higher MACE.</p><p><strong>Conclusion: </strong>In conclusion, the study found that patients with both CVD and active cancer suffered relatively worse outcomes when they had acute SARS-CoV-2 infection during early and alpha surges in the United States. These findings highlight the need for improved management strategies and further research to better understand the impact of the virus on vulnerable populations during the COVID-19 pandemic.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"9 1","pages":"36"},"PeriodicalIF":3.2000,"publicationDate":"2023-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10557272/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes of patients with active cancers and pre-existing cardiovascular diseases infected with SARS-CoV-2.\",\"authors\":\"Brijesh Patel, Scott A Chapman, Jake T Neumann, Aayush Visaria, Oluwabunmi Ogungbe, Sijin Wen, Maryam Khodaverdi, Priyal Makwana, Jasvinder A Singh, George Sokos\",\"doi\":\"10.1186/s40959-023-00187-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To determine the impact of acute SARS-CoV-2 infection on patient with concomitant active cancer and CVD.</p><p><strong>Methods: </strong>The researchers extracted and analyzed data from the National COVID Cohort Collaborative (N3C) database between January 1, 2020, and July 22, 2022. They included only patients with acute SARS-CoV-2 infection, defined as a positive test by PCR 21 days before and 5 days after the day of index hospitalization. Active cancers were defined as last cancer drug administered within 30 days of index admission. The \\\"Cardioonc\\\" group consisted of patients with CVD and active cancers. The cohort was divided into four groups: (1) CVD (-), (2) CVD ( +), (3) Cardioonc (-), and (4) Cardioonc ( +), where (-) or ( +) denotes acute SARS-CoV-2 infection status. The primary outcome of the study was major adverse cardiovascular events (MACE), including acute stroke, acute heart failure, myocardial infarction, or all-cause mortality. The researchers analyzed the outcomes by different phases of the pandemic and performed competing-risk analysis for other MACE components and death as a competing event.</p><p><strong>Results: </strong>The study analyzed 418,306 patients, of which 74%, 10%, 15.7%, and 0.3% had CVD (-), CVD ( +), Cardioonc (-), and Cardioonc ( +), respectively. The Cardioonc ( +) group had the highest MACE events in all four phases of the pandemic. Compared to CVD (-), the Cardioonc ( +) group had an odds ratio of 1.66 for MACE. However, during the Omicron era, there was a statistically significant increased risk for MACE in the Cardioonc ( +) group compared to CVD (-). Competing risk analysis showed that all-cause mortality was significantly higher in the Cardioonc ( +) group and limited other MACE events from occurring. When the researchers identified specific cancer types, patients with colon cancer had higher MACE.</p><p><strong>Conclusion: </strong>In conclusion, the study found that patients with both CVD and active cancer suffered relatively worse outcomes when they had acute SARS-CoV-2 infection during early and alpha surges in the United States. These findings highlight the need for improved management strategies and further research to better understand the impact of the virus on vulnerable populations during the COVID-19 pandemic.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"9 1\",\"pages\":\"36\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2023-10-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10557272/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-023-00187-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-023-00187-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Outcomes of patients with active cancers and pre-existing cardiovascular diseases infected with SARS-CoV-2.
Objective: To determine the impact of acute SARS-CoV-2 infection on patient with concomitant active cancer and CVD.
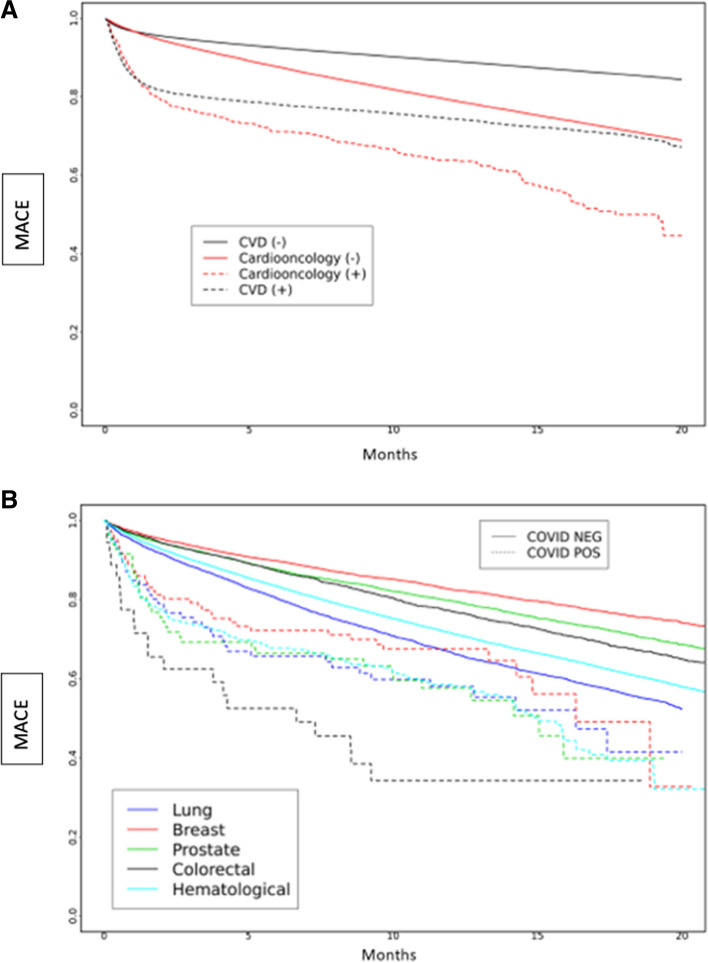
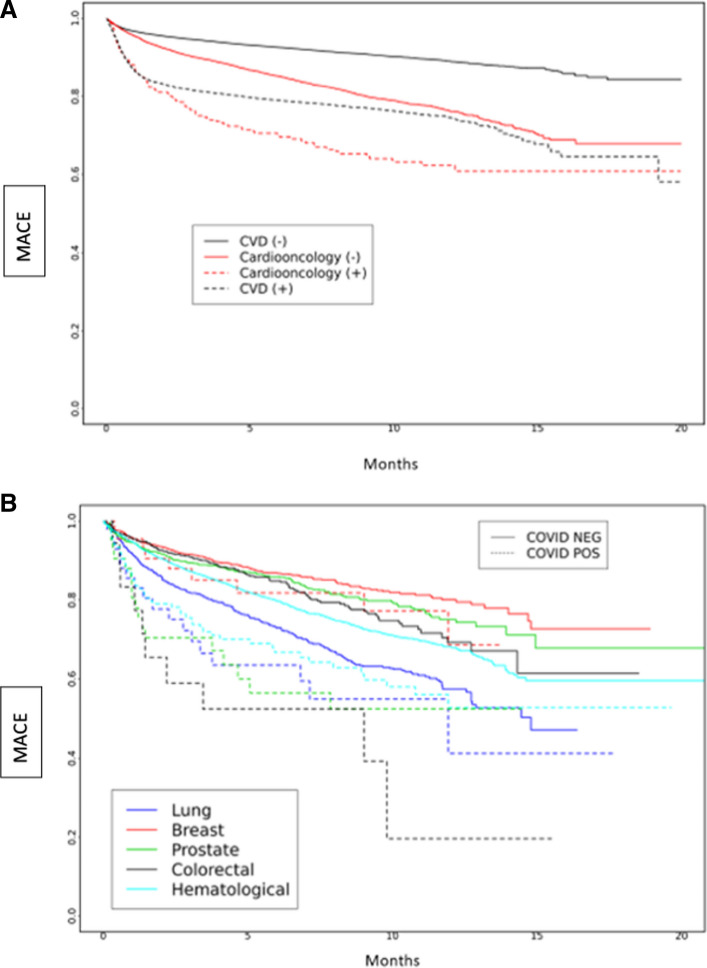
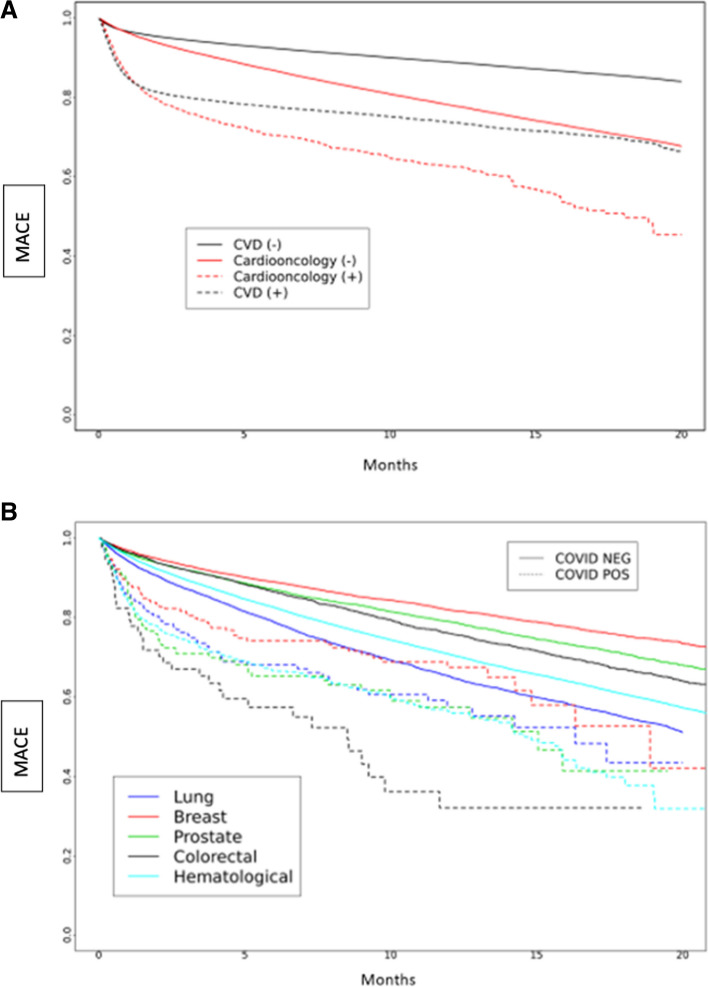
Methods: The researchers extracted and analyzed data from the National COVID Cohort Collaborative (N3C) database between January 1, 2020, and July 22, 2022. They included only patients with acute SARS-CoV-2 infection, defined as a positive test by PCR 21 days before and 5 days after the day of index hospitalization. Active cancers were defined as last cancer drug administered within 30 days of index admission. The "Cardioonc" group consisted of patients with CVD and active cancers. The cohort was divided into four groups: (1) CVD (-), (2) CVD ( +), (3) Cardioonc (-), and (4) Cardioonc ( +), where (-) or ( +) denotes acute SARS-CoV-2 infection status. The primary outcome of the study was major adverse cardiovascular events (MACE), including acute stroke, acute heart failure, myocardial infarction, or all-cause mortality. The researchers analyzed the outcomes by different phases of the pandemic and performed competing-risk analysis for other MACE components and death as a competing event.
Results: The study analyzed 418,306 patients, of which 74%, 10%, 15.7%, and 0.3% had CVD (-), CVD ( +), Cardioonc (-), and Cardioonc ( +), respectively. The Cardioonc ( +) group had the highest MACE events in all four phases of the pandemic. Compared to CVD (-), the Cardioonc ( +) group had an odds ratio of 1.66 for MACE. However, during the Omicron era, there was a statistically significant increased risk for MACE in the Cardioonc ( +) group compared to CVD (-). Competing risk analysis showed that all-cause mortality was significantly higher in the Cardioonc ( +) group and limited other MACE events from occurring. When the researchers identified specific cancer types, patients with colon cancer had higher MACE.
Conclusion: In conclusion, the study found that patients with both CVD and active cancer suffered relatively worse outcomes when they had acute SARS-CoV-2 infection during early and alpha surges in the United States. These findings highlight the need for improved management strategies and further research to better understand the impact of the virus on vulnerable populations during the COVID-19 pandemic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


