{"title":"血清半乳糖凝集素-3预测静脉动脉体外膜肺氧合患者的死亡率。","authors":"Jianlong Zhu, Dehui Guo, Liying Liu, Jing Zhong","doi":"10.1155/2023/3917156","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We investigated the potential use of galectin-3 (Gal-3) as a prognostic indicator for patients with cardiogenic shock and developed a predictive mortality model for venoarterial extracorporeal membrane oxygenation (VA-ECMO).</p><p><strong>Methods: </strong>We prospectively studied patients (survivors and nonsurvivors) who received VA-ECMO for cardiogenic shock from 2019 to 2021. We recorded baseline data, Gal-3, and B-type natriuretic peptide (BNP) before ECMO and 24-72 h after ECMO. We used multivariable logistic regression to analyze significant risk factors and construct a VA-ECMO death prediction model. Receiver operating characteristic (ROC) curves were plotted to assess the predictive efficacy of the model.</p><p><strong>Results: </strong>We enrolled 73 patients with cardiogenic shock who received VA-ECMO support; 38 (52.05%) died in hospital. The median age was 57 years (interquartile range (IQR): 48-67 years); the median duration of ECMO therapy was 5.8 days (IQR: 4.62-7.57 days); and the median intensive care unit stay was 19.04 days (IQR: 13.92-26.15 days). Compared with the nonsurvivors, survivors had lower acute physiology and chronic health evaluation (APACHE) II scores (<i>p</i> < 0.001), increased left ventricular ejection fraction (<i>p</i> < 0.05), lower Gal-3 levels at 24 and 72 h (both <i>p</i> = 0.001), lower BNP levels at 24 and 72 h (both <i>p</i> = 0.001), and higher platelet counts (<i>p</i> = 0.009). Further multivariable analysis showed that APACHE II score, BNP-T72, and Gal-3-T72 were independent risk factors for death in VA-ECMO patients. Gal-3 and BNP were positively correlated (<i>p</i> < 0.05) and decreased significantly during ECMO treatment. The areas under the ROC curve (AUC) for APACHE II score, Gal-3-T72, and BNP-T72 were 0.687, 0.799, and 0.723, respectively. We constructed a combined prediction model with an AUC of 0.884 (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>Gal-3 may serve as a prognostic indicator for patients receiving VA-ECMO for cardiogenic shock. The combined early warning score is a simple and effective tool for predicting mortality in VA-ECMO patients.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2023 ","pages":"3917156"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10560122/pdf/","citationCount":"0","resultStr":"{\"title\":\"Serum Galectin-3 Predicts Mortality in Venoarterial Extracorporeal Membrane Oxygenation Patients.\",\"authors\":\"Jianlong Zhu, Dehui Guo, Liying Liu, Jing Zhong\",\"doi\":\"10.1155/2023/3917156\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>We investigated the potential use of galectin-3 (Gal-3) as a prognostic indicator for patients with cardiogenic shock and developed a predictive mortality model for venoarterial extracorporeal membrane oxygenation (VA-ECMO).</p><p><strong>Methods: </strong>We prospectively studied patients (survivors and nonsurvivors) who received VA-ECMO for cardiogenic shock from 2019 to 2021. We recorded baseline data, Gal-3, and B-type natriuretic peptide (BNP) before ECMO and 24-72 h after ECMO. We used multivariable logistic regression to analyze significant risk factors and construct a VA-ECMO death prediction model. Receiver operating characteristic (ROC) curves were plotted to assess the predictive efficacy of the model.</p><p><strong>Results: </strong>We enrolled 73 patients with cardiogenic shock who received VA-ECMO support; 38 (52.05%) died in hospital. The median age was 57 years (interquartile range (IQR): 48-67 years); the median duration of ECMO therapy was 5.8 days (IQR: 4.62-7.57 days); and the median intensive care unit stay was 19.04 days (IQR: 13.92-26.15 days). Compared with the nonsurvivors, survivors had lower acute physiology and chronic health evaluation (APACHE) II scores (<i>p</i> < 0.001), increased left ventricular ejection fraction (<i>p</i> < 0.05), lower Gal-3 levels at 24 and 72 h (both <i>p</i> = 0.001), lower BNP levels at 24 and 72 h (both <i>p</i> = 0.001), and higher platelet counts (<i>p</i> = 0.009). Further multivariable analysis showed that APACHE II score, BNP-T72, and Gal-3-T72 were independent risk factors for death in VA-ECMO patients. Gal-3 and BNP were positively correlated (<i>p</i> < 0.05) and decreased significantly during ECMO treatment. The areas under the ROC curve (AUC) for APACHE II score, Gal-3-T72, and BNP-T72 were 0.687, 0.799, and 0.723, respectively. We constructed a combined prediction model with an AUC of 0.884 (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>Gal-3 may serve as a prognostic indicator for patients receiving VA-ECMO for cardiogenic shock. The combined early warning score is a simple and effective tool for predicting mortality in VA-ECMO patients.</p>\",\"PeriodicalId\":9494,\"journal\":{\"name\":\"Cardiology Research and Practice\",\"volume\":\"2023 \",\"pages\":\"3917156\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10560122/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research and Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/3917156\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/3917156","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:我们研究了半乳糖凝集素-3(Gal-3)作为心源性休克患者预后指标的潜在用途,并建立了体外膜肺氧合(VA-ECMO)的预测死亡率模型。方法:我们前瞻性研究了2019年至2021年接受VA-ECMO治疗心源性休克的患者(幸存者和非幸存者)。我们记录了ECMO和24-72前的基线数据、Gal-3和B型钠尿肽(BNP) ECMO后h。我们使用多变量逻辑回归来分析显著的风险因素,并构建VA-ECMO死亡预测模型。绘制受试者工作特性(ROC)曲线以评估模型的预测功效。结果:我们纳入了73例接受VA-ECMO支持的心源性休克患者;38例(52.05%)在医院死亡。中位年龄为57岁 年(四分位间距(IQR):48-67 年);ECMO治疗的中位持续时间为5.8 天(IQR:4.62-7.57 天);重症监护病房的平均住院时间为19.04 天(IQR:13.92-26.15 天)。与非幸存者相比,幸存者的急性生理学和慢性健康评估(APACHE)II评分较低(p p p = 0.001),24和72时的BNP水平较低 h(两个p = 0.001)和较高的血小板计数(p = 0.009)。进一步的多变量分析显示,APACHE II评分、BNP-T72和Gal-3-T72是VA-ECMO患者死亡的独立危险因素。Gal-3与BNP呈正相关(p p 结论:Gal-3可作为VA-ECMO治疗心源性休克患者的预后指标。联合预警评分是预测VA-ECMO患者死亡率的一种简单有效的工具。
Serum Galectin-3 Predicts Mortality in Venoarterial Extracorporeal Membrane Oxygenation Patients.
Objective: We investigated the potential use of galectin-3 (Gal-3) as a prognostic indicator for patients with cardiogenic shock and developed a predictive mortality model for venoarterial extracorporeal membrane oxygenation (VA-ECMO).
Methods: We prospectively studied patients (survivors and nonsurvivors) who received VA-ECMO for cardiogenic shock from 2019 to 2021. We recorded baseline data, Gal-3, and B-type natriuretic peptide (BNP) before ECMO and 24-72 h after ECMO. We used multivariable logistic regression to analyze significant risk factors and construct a VA-ECMO death prediction model. Receiver operating characteristic (ROC) curves were plotted to assess the predictive efficacy of the model.
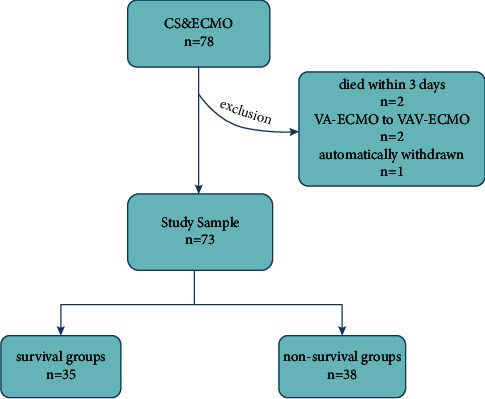
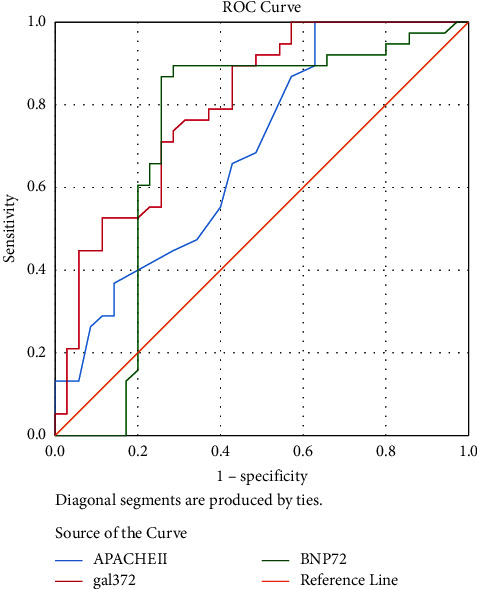
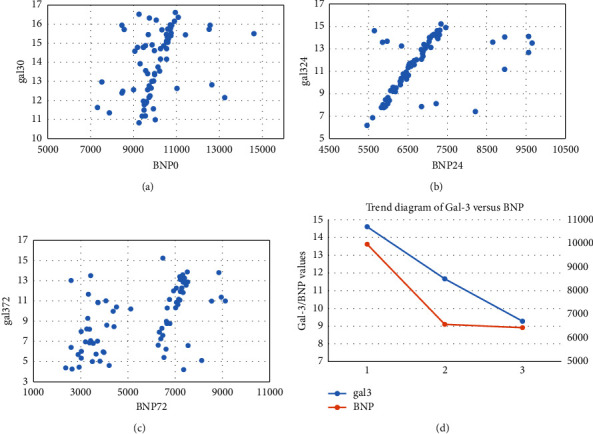
Results: We enrolled 73 patients with cardiogenic shock who received VA-ECMO support; 38 (52.05%) died in hospital. The median age was 57 years (interquartile range (IQR): 48-67 years); the median duration of ECMO therapy was 5.8 days (IQR: 4.62-7.57 days); and the median intensive care unit stay was 19.04 days (IQR: 13.92-26.15 days). Compared with the nonsurvivors, survivors had lower acute physiology and chronic health evaluation (APACHE) II scores (p < 0.001), increased left ventricular ejection fraction (p < 0.05), lower Gal-3 levels at 24 and 72 h (both p = 0.001), lower BNP levels at 24 and 72 h (both p = 0.001), and higher platelet counts (p = 0.009). Further multivariable analysis showed that APACHE II score, BNP-T72, and Gal-3-T72 were independent risk factors for death in VA-ECMO patients. Gal-3 and BNP were positively correlated (p < 0.05) and decreased significantly during ECMO treatment. The areas under the ROC curve (AUC) for APACHE II score, Gal-3-T72, and BNP-T72 were 0.687, 0.799, and 0.723, respectively. We constructed a combined prediction model with an AUC of 0.884 (p < 0.01).
Conclusion: Gal-3 may serve as a prognostic indicator for patients receiving VA-ECMO for cardiogenic shock. The combined early warning score is a simple and effective tool for predicting mortality in VA-ECMO patients.
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


