Behoavy Mahafaly Ralaizanaka, Chantelli Iamblaudiot Razafindrazoto, Eloïse Bolot, Georges Bors, Stéphanie Housson-Wetzel, Soloniaina Hélio Razafimahefa, Rado Manitrala Ramanampamonjy, Pierre Claude
{"title":"胃肠道粘液霉菌病引起的大量下消化道出血、直肠穿孔和肺栓塞:一个病例报告的漫长诊断途径。","authors":"Behoavy Mahafaly Ralaizanaka, Chantelli Iamblaudiot Razafindrazoto, Eloïse Bolot, Georges Bors, Stéphanie Housson-Wetzel, Soloniaina Hélio Razafimahefa, Rado Manitrala Ramanampamonjy, Pierre Claude","doi":"10.2147/CEG.S373728","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Mucormycosis is a rare systemic fungal infection, mainly observed in immunocompromised patients. It is responsible for surface and deep tissue destruction leading to perforations and hemorrhage. Its pathogenesis represented by an angio-invasion is at the origin of a local infarction and a vascular thrombosis. We report a case of gastrointestinal (GI) mucormycosis-induced multiple gastric ulcers, GI bleeding and rectal perforation.</p><p><strong>Case presentation: </strong>A 75-year-old man, with type II diabetes mellitus, was admitted to the intensive care unit for an acute abdominal pain associated with massive hematochezia. Clinical examination was that of an acute peritonitis and a hemorrhagic shock state. Abdominal and pelvic CT scan with intravenous contrast concluded to a perforation of the anterior wall of the rectum. He underwent immediate laparotomy with temporary colostomy. Several upper GI endoscopies had shown multiple gastric ulcer lesions. Lower GI endoscopy showed a fistulous orifice of the rectum on its anterior surface. Histopathology of the gastric biopsy showed acute and subacute inflammatory changes with filamentous elements suggesting mucormycosis. Histopathology of the rectal biopsy showed a subacute non-specific inflammation. Culture of the secretions from the rectal fistula orifice showed the strain <i>Rhizopus</i> sp. Antifungal susceptibility testing reported sensitivity to liposomal amphotericin B. The diagnosis of GI mucormycosis-induced multiple gastric ulcers, rectal perforation and pulmonary embolism in the patient with type II diabetes mellitus was retained. The outcomes were favorable after 6 weeks of treatment with liposomal amphotericin B associated with temporary colostomy and appropriate diabetes management.</p><p><strong>Conclusion: </strong>GI mucormycosis remains a multidisciplinary diagnostic challenge, less frequent in clinical practice, with a long diagnostic pathway. This opportunistic systemic mycosis can lead to numerous GI complications including perforation, massive GI bleeding and even multiple extra-GI complications. GI mucormycosis has a good prognosis if it is treated early with medical and surgical treatment.</p>","PeriodicalId":10208,"journal":{"name":"Clinical and Experimental Gastroenterology","volume":" ","pages":"145-151"},"PeriodicalIF":2.5000,"publicationDate":"2022-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/ec/ceg-15-145.PMC9381012.pdf","citationCount":"0","resultStr":"{\"title\":\"Gastrointestinal Mucormycosis-Induced Massive Lower Gastrointestinal Bleeding, Rectal Perforation, and Pulmonary Embolism: A Long Diagnostic Pathway in a Case Report.\",\"authors\":\"Behoavy Mahafaly Ralaizanaka, Chantelli Iamblaudiot Razafindrazoto, Eloïse Bolot, Georges Bors, Stéphanie Housson-Wetzel, Soloniaina Hélio Razafimahefa, Rado Manitrala Ramanampamonjy, Pierre Claude\",\"doi\":\"10.2147/CEG.S373728\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Mucormycosis is a rare systemic fungal infection, mainly observed in immunocompromised patients. It is responsible for surface and deep tissue destruction leading to perforations and hemorrhage. Its pathogenesis represented by an angio-invasion is at the origin of a local infarction and a vascular thrombosis. We report a case of gastrointestinal (GI) mucormycosis-induced multiple gastric ulcers, GI bleeding and rectal perforation.</p><p><strong>Case presentation: </strong>A 75-year-old man, with type II diabetes mellitus, was admitted to the intensive care unit for an acute abdominal pain associated with massive hematochezia. Clinical examination was that of an acute peritonitis and a hemorrhagic shock state. Abdominal and pelvic CT scan with intravenous contrast concluded to a perforation of the anterior wall of the rectum. He underwent immediate laparotomy with temporary colostomy. Several upper GI endoscopies had shown multiple gastric ulcer lesions. Lower GI endoscopy showed a fistulous orifice of the rectum on its anterior surface. Histopathology of the gastric biopsy showed acute and subacute inflammatory changes with filamentous elements suggesting mucormycosis. Histopathology of the rectal biopsy showed a subacute non-specific inflammation. Culture of the secretions from the rectal fistula orifice showed the strain <i>Rhizopus</i> sp. Antifungal susceptibility testing reported sensitivity to liposomal amphotericin B. The diagnosis of GI mucormycosis-induced multiple gastric ulcers, rectal perforation and pulmonary embolism in the patient with type II diabetes mellitus was retained. The outcomes were favorable after 6 weeks of treatment with liposomal amphotericin B associated with temporary colostomy and appropriate diabetes management.</p><p><strong>Conclusion: </strong>GI mucormycosis remains a multidisciplinary diagnostic challenge, less frequent in clinical practice, with a long diagnostic pathway. This opportunistic systemic mycosis can lead to numerous GI complications including perforation, massive GI bleeding and even multiple extra-GI complications. GI mucormycosis has a good prognosis if it is treated early with medical and surgical treatment.</p>\",\"PeriodicalId\":10208,\"journal\":{\"name\":\"Clinical and Experimental Gastroenterology\",\"volume\":\" \",\"pages\":\"145-151\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2022-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/ec/ceg-15-145.PMC9381012.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEG.S373728\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEG.S373728","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Gastrointestinal Mucormycosis-Induced Massive Lower Gastrointestinal Bleeding, Rectal Perforation, and Pulmonary Embolism: A Long Diagnostic Pathway in a Case Report.
Introduction: Mucormycosis is a rare systemic fungal infection, mainly observed in immunocompromised patients. It is responsible for surface and deep tissue destruction leading to perforations and hemorrhage. Its pathogenesis represented by an angio-invasion is at the origin of a local infarction and a vascular thrombosis. We report a case of gastrointestinal (GI) mucormycosis-induced multiple gastric ulcers, GI bleeding and rectal perforation.
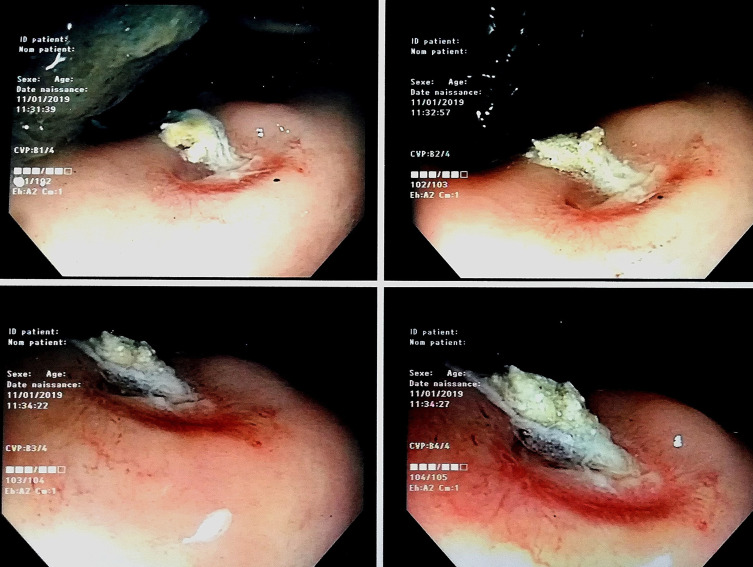
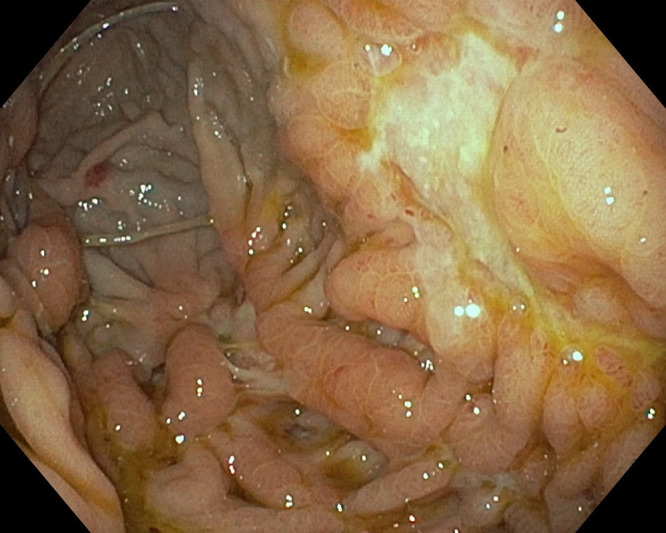
Case presentation: A 75-year-old man, with type II diabetes mellitus, was admitted to the intensive care unit for an acute abdominal pain associated with massive hematochezia. Clinical examination was that of an acute peritonitis and a hemorrhagic shock state. Abdominal and pelvic CT scan with intravenous contrast concluded to a perforation of the anterior wall of the rectum. He underwent immediate laparotomy with temporary colostomy. Several upper GI endoscopies had shown multiple gastric ulcer lesions. Lower GI endoscopy showed a fistulous orifice of the rectum on its anterior surface. Histopathology of the gastric biopsy showed acute and subacute inflammatory changes with filamentous elements suggesting mucormycosis. Histopathology of the rectal biopsy showed a subacute non-specific inflammation. Culture of the secretions from the rectal fistula orifice showed the strain Rhizopus sp. Antifungal susceptibility testing reported sensitivity to liposomal amphotericin B. The diagnosis of GI mucormycosis-induced multiple gastric ulcers, rectal perforation and pulmonary embolism in the patient with type II diabetes mellitus was retained. The outcomes were favorable after 6 weeks of treatment with liposomal amphotericin B associated with temporary colostomy and appropriate diabetes management.
Conclusion: GI mucormycosis remains a multidisciplinary diagnostic challenge, less frequent in clinical practice, with a long diagnostic pathway. This opportunistic systemic mycosis can lead to numerous GI complications including perforation, massive GI bleeding and even multiple extra-GI complications. GI mucormycosis has a good prognosis if it is treated early with medical and surgical treatment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


