{"title":"大麻与慢性阻塞性肺病和新冠肺炎感染的关联。","authors":"Steven Lehrer, Peter H. Rheinstein","doi":"10.1002/cdt3.38","DOIUrl":null,"url":null,"abstract":"<p>In a 2012 study, occasional and low cumulative cannabis use was not associated with adverse effects on pulmonary function.<span><sup>1</sup></span> With tobacco, the more used, the more loss of air flow rate and lung volume. The same was not true with cannabis use. Air flow rate increased rather than decreased with increased exposure to cannabis up to a certain level.</p><p>An important factor that helped explain the difference in effects from tobacco and cannabis was the amount of each that was smoked. Tobacco users typically smoked 10–20 cigarettes daily, some even more. Cannabis smokers, on average, smoked only two to three times a month, so the average exposure to cannabis was much lower than for tobacco. People experiment with cannabis in their late teens and 20s, and some consume relatively low levels for years. Although heavy exposure to cannabis might damage the lungs, reliable estimates of the effects of heavy use were not available in the 2012 study, as heavy users were relatively rare in the study population.</p><p>In the current analysis, we used data from UK Biobank (UKB) to assess the effect of cannabis on coronavirus disease (COVID-19) infection and to determine whether cannabis lung damage might facilitate COVID-19 infection in formerly heavy users.</p><p>The UKB is a large prospective observational study comprising about 500,000 men and women (<i>N</i> = 229,134 men, <i>N</i> = 273,402 women), more than 90% White, aged 40–69 years at enrollment. Participants were recruited from across 22 centers located throughout England, Wales, and Scotland, between 2006 and 2010, and continue to be longitudinally followed for capture of subsequent health events.<span><sup>2</sup></span> This methodology is like that of the Framingham Heart Study,<span><sup>3</sup></span> with the exception that the UKB program collects postmortem samples, which Framingham did not.</p><p>Our UKB application was approved as UKB project 57,245 (S.L. and P.H.R.).</p><p>Doctor-diagnosed chronic obstructive pulmonary disease (COPD) is from UKB data field 22,130. At enrollment, the subject was asked on a touchscreen, “Has a doctor ever told you that you have had any of the conditions below?” COPD was one of the options listed.</p><p>The subject was asked, “Have you taken cannabis (marijuana, grass, hash, ganja, blow, draw, skunk, weed, spliff, dope), even if it was a long time ago?” If the answer was “yes,” cannabis use was recorded in the UKB data field 20,454, maximum frequency of taking cannabis, question asked: “Considering when you were taking cannabis most regularly, how often did you take it?” Answers were 1 = <i>Less than once a month</i>, 2 = <i>Once a month or more, but not every week</i>, 3 = <i>Once a week or more, but not every day</i>, and 4 = <i>Every day</i>. Subject was then asked (UKB data field 20455) “About how old were you when you last had cannabis?”</p><p>All UKB subjects who had cannabis-use data, COVID-19 test data, and COPD data were included in the study.</p><p>Electronic linkage between UKB records and National Health Service COVID-19 laboratory test results in England were available from March 16 to April 26, 2020, including the peak of daily COVID-19 laboratory-confirmed cases in the current outbreak. During this period, testing of older groups was largely restricted to hospital inpatients with clinical signs of infection, so test positivity is considered a good marker of severe COVID-19.<span><sup>4</sup></span></p><p>Data processing was performed on Minerva, a Linux mainframe with Centos 7.6, at the Icahn School of Medicine at Mount Sinai. We used the UKB Data Parser (ukbb parser), a python-based package that allows easy interfacing with the large UKB data set.<span><sup>5</sup></span></p><p>Mean age of subjects was 57 ± 8.1 (mean ± SD). Fifty-four percent were women and 46% were men. Ninety-eight percent were White British. Subjects had not smoked cannabis for 24 ± 11 years (Figure 1).</p><p>Cannabis maximum use versus COPD incidence in 20,996 subjects is shown in Table 1. Increasing cannabis use was associated with increased COPD prevalence (<i>p</i> = 0.011, Fisher's exact test, two tailed).</p><p>COVID-19 test result versus ever-taking cannabis is shown in Table 2. Increased cannabis use was associated with increased COVID-19 test positivity (<i>p</i> = 0.026, Fisher's exact test, two tailed).</p><p>Table 3 shows logistic regression, COVID-19 test result, dependent variable, ever-taking cannabis, pack-years smoking, and independent variables. The effects of cannabis and pack-years smoking on COVID-19 test result were significant and independent.</p><p>Tobacco smoking increases the risk of lung infections, possibly including COVID-19. Smoking impairs the immune system and almost doubles the risk of tuberculosis. Smoking affects macrophages and cytokine response, and therefore the ability to contain infection. The risk for pneumococcal, legionella, and mycoplasma pneumonia infection is about three to five times higher in smokers.<span><sup>6</sup></span> In one study, current smokers were more likely to report symptoms, suggesting a diagnosis of COVID-19.<span><sup>7</sup></span></p><p>The effects of smoking cannabis are difficult to assess accurately and to distinguish from the effects of tobacco; nevertheless, cannabis use may cause severe lung damage. Cannabis smoke affects the lungs similarly to tobacco smoke, causing symptoms such as increased cough, sputum, and hyperinflation. Cannabis can produce serious lung diseases with increasing years of use. Cannabis may weaken the immune system, leading to pneumonia. Smoking cannabis has been linked to symptoms of chronic bronchitis. Heavy use of cannabis can result in airway obstruction<span><sup>8</sup></span> and worse COVID-19 outcome.<span><sup>9</sup></span> Yet, cannabis use might reduce lung inflammation and inhibit viral replication<span><sup>10</sup></span> in Covid-19 infections, leading to a better outcome in some cases.<span><sup>11, 12</sup></span></p><p>As noted above, we found that the effects of cannabis and pack-years smoking on COVID-19 test result were significant and independent (Table 3). This suggests that the damaging effects of cannabis and smoking on the lung are additive, even though cannabis had not been smoked for a decade or more.</p><p>Our study has weaknesses. COVID-19-positive test results were related to cannabis use (Table 2). However, we did not have data relating the frequency of cannabis use to susceptibility COVID-19. In the logistic regression (Table 3), more independent variables would be worthwhile. Moreover, the high incidence of Caucasian subjects might influence the results.</p><p>It is never too late to quit smoking tobacco. As soon as a tobacco smoker quits, his chances are diminished of getting cancer and other diseases.<span><sup>13</sup></span> Our findings imply that cannabis may be similar. Fifteen years after quitting tobacco, risk of coronary heart disease is close to that of a nonsmoker.<span><sup>14</sup></span> Unlike the heart, the lung does not forget the insult from inhaled tobacco or cannabis, even many years later, but after quitting the lung damage may not further increase.</p><p>Changes in cannabis policies across states legalizing it for medical and recreational use suggest that cannabis is winning increased acceptance in our society. Thus, people must understand what is known about the adverse health effects of cannabis.<span><sup>15</sup></span> As cannabis use becomes more widespread, no doubt more adverse effects will come to light.</p><p>Steven Lehrer and Peter H. Rheinstein contributed equally to this study.</p><p>The authors declare no conflict of interest.</p><p>UK Biobank has approval from the Northwest Multi-center Research Ethics Committee (MREC), which covers the United Kingdom. It also sought the approval in England and Wales from the Patient Information Advisory Group (PIAG) for gaining access to information that would allow it to invite people to participate. PIAG has since been replaced by the National Information Governance Board for Health & Social Care (NIGB). In Scotland, UK Biobank has approval from the Community Health Index Advisory Group (CHIAG).</p>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"8 3","pages":"238-241"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/56/d2/CDT3-8-238.PMC9349800.pdf","citationCount":"1","resultStr":"{\"title\":\"Association of cannabis with chronic obstructive pulmonary disease and COVID-19 infection\",\"authors\":\"Steven Lehrer, Peter H. Rheinstein\",\"doi\":\"10.1002/cdt3.38\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In a 2012 study, occasional and low cumulative cannabis use was not associated with adverse effects on pulmonary function.<span><sup>1</sup></span> With tobacco, the more used, the more loss of air flow rate and lung volume. The same was not true with cannabis use. Air flow rate increased rather than decreased with increased exposure to cannabis up to a certain level.</p><p>An important factor that helped explain the difference in effects from tobacco and cannabis was the amount of each that was smoked. Tobacco users typically smoked 10–20 cigarettes daily, some even more. Cannabis smokers, on average, smoked only two to three times a month, so the average exposure to cannabis was much lower than for tobacco. People experiment with cannabis in their late teens and 20s, and some consume relatively low levels for years. Although heavy exposure to cannabis might damage the lungs, reliable estimates of the effects of heavy use were not available in the 2012 study, as heavy users were relatively rare in the study population.</p><p>In the current analysis, we used data from UK Biobank (UKB) to assess the effect of cannabis on coronavirus disease (COVID-19) infection and to determine whether cannabis lung damage might facilitate COVID-19 infection in formerly heavy users.</p><p>The UKB is a large prospective observational study comprising about 500,000 men and women (<i>N</i> = 229,134 men, <i>N</i> = 273,402 women), more than 90% White, aged 40–69 years at enrollment. Participants were recruited from across 22 centers located throughout England, Wales, and Scotland, between 2006 and 2010, and continue to be longitudinally followed for capture of subsequent health events.<span><sup>2</sup></span> This methodology is like that of the Framingham Heart Study,<span><sup>3</sup></span> with the exception that the UKB program collects postmortem samples, which Framingham did not.</p><p>Our UKB application was approved as UKB project 57,245 (S.L. and P.H.R.).</p><p>Doctor-diagnosed chronic obstructive pulmonary disease (COPD) is from UKB data field 22,130. At enrollment, the subject was asked on a touchscreen, “Has a doctor ever told you that you have had any of the conditions below?” COPD was one of the options listed.</p><p>The subject was asked, “Have you taken cannabis (marijuana, grass, hash, ganja, blow, draw, skunk, weed, spliff, dope), even if it was a long time ago?” If the answer was “yes,” cannabis use was recorded in the UKB data field 20,454, maximum frequency of taking cannabis, question asked: “Considering when you were taking cannabis most regularly, how often did you take it?” Answers were 1 = <i>Less than once a month</i>, 2 = <i>Once a month or more, but not every week</i>, 3 = <i>Once a week or more, but not every day</i>, and 4 = <i>Every day</i>. Subject was then asked (UKB data field 20455) “About how old were you when you last had cannabis?”</p><p>All UKB subjects who had cannabis-use data, COVID-19 test data, and COPD data were included in the study.</p><p>Electronic linkage between UKB records and National Health Service COVID-19 laboratory test results in England were available from March 16 to April 26, 2020, including the peak of daily COVID-19 laboratory-confirmed cases in the current outbreak. During this period, testing of older groups was largely restricted to hospital inpatients with clinical signs of infection, so test positivity is considered a good marker of severe COVID-19.<span><sup>4</sup></span></p><p>Data processing was performed on Minerva, a Linux mainframe with Centos 7.6, at the Icahn School of Medicine at Mount Sinai. We used the UKB Data Parser (ukbb parser), a python-based package that allows easy interfacing with the large UKB data set.<span><sup>5</sup></span></p><p>Mean age of subjects was 57 ± 8.1 (mean ± SD). Fifty-four percent were women and 46% were men. Ninety-eight percent were White British. Subjects had not smoked cannabis for 24 ± 11 years (Figure 1).</p><p>Cannabis maximum use versus COPD incidence in 20,996 subjects is shown in Table 1. Increasing cannabis use was associated with increased COPD prevalence (<i>p</i> = 0.011, Fisher's exact test, two tailed).</p><p>COVID-19 test result versus ever-taking cannabis is shown in Table 2. Increased cannabis use was associated with increased COVID-19 test positivity (<i>p</i> = 0.026, Fisher's exact test, two tailed).</p><p>Table 3 shows logistic regression, COVID-19 test result, dependent variable, ever-taking cannabis, pack-years smoking, and independent variables. The effects of cannabis and pack-years smoking on COVID-19 test result were significant and independent.</p><p>Tobacco smoking increases the risk of lung infections, possibly including COVID-19. Smoking impairs the immune system and almost doubles the risk of tuberculosis. Smoking affects macrophages and cytokine response, and therefore the ability to contain infection. The risk for pneumococcal, legionella, and mycoplasma pneumonia infection is about three to five times higher in smokers.<span><sup>6</sup></span> In one study, current smokers were more likely to report symptoms, suggesting a diagnosis of COVID-19.<span><sup>7</sup></span></p><p>The effects of smoking cannabis are difficult to assess accurately and to distinguish from the effects of tobacco; nevertheless, cannabis use may cause severe lung damage. Cannabis smoke affects the lungs similarly to tobacco smoke, causing symptoms such as increased cough, sputum, and hyperinflation. Cannabis can produce serious lung diseases with increasing years of use. Cannabis may weaken the immune system, leading to pneumonia. Smoking cannabis has been linked to symptoms of chronic bronchitis. Heavy use of cannabis can result in airway obstruction<span><sup>8</sup></span> and worse COVID-19 outcome.<span><sup>9</sup></span> Yet, cannabis use might reduce lung inflammation and inhibit viral replication<span><sup>10</sup></span> in Covid-19 infections, leading to a better outcome in some cases.<span><sup>11, 12</sup></span></p><p>As noted above, we found that the effects of cannabis and pack-years smoking on COVID-19 test result were significant and independent (Table 3). This suggests that the damaging effects of cannabis and smoking on the lung are additive, even though cannabis had not been smoked for a decade or more.</p><p>Our study has weaknesses. COVID-19-positive test results were related to cannabis use (Table 2). However, we did not have data relating the frequency of cannabis use to susceptibility COVID-19. In the logistic regression (Table 3), more independent variables would be worthwhile. Moreover, the high incidence of Caucasian subjects might influence the results.</p><p>It is never too late to quit smoking tobacco. As soon as a tobacco smoker quits, his chances are diminished of getting cancer and other diseases.<span><sup>13</sup></span> Our findings imply that cannabis may be similar. Fifteen years after quitting tobacco, risk of coronary heart disease is close to that of a nonsmoker.<span><sup>14</sup></span> Unlike the heart, the lung does not forget the insult from inhaled tobacco or cannabis, even many years later, but after quitting the lung damage may not further increase.</p><p>Changes in cannabis policies across states legalizing it for medical and recreational use suggest that cannabis is winning increased acceptance in our society. Thus, people must understand what is known about the adverse health effects of cannabis.<span><sup>15</sup></span> As cannabis use becomes more widespread, no doubt more adverse effects will come to light.</p><p>Steven Lehrer and Peter H. Rheinstein contributed equally to this study.</p><p>The authors declare no conflict of interest.</p><p>UK Biobank has approval from the Northwest Multi-center Research Ethics Committee (MREC), which covers the United Kingdom. It also sought the approval in England and Wales from the Patient Information Advisory Group (PIAG) for gaining access to information that would allow it to invite people to participate. PIAG has since been replaced by the National Information Governance Board for Health & Social Care (NIGB). In Scotland, UK Biobank has approval from the Community Health Index Advisory Group (CHIAG).</p>\",\"PeriodicalId\":32096,\"journal\":{\"name\":\"Chronic Diseases and Translational Medicine\",\"volume\":\"8 3\",\"pages\":\"238-241\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-06-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/56/d2/CDT3-8-238.PMC9349800.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chronic Diseases and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.38\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.38","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Association of cannabis with chronic obstructive pulmonary disease and COVID-19 infection
In a 2012 study, occasional and low cumulative cannabis use was not associated with adverse effects on pulmonary function.1 With tobacco, the more used, the more loss of air flow rate and lung volume. The same was not true with cannabis use. Air flow rate increased rather than decreased with increased exposure to cannabis up to a certain level.
An important factor that helped explain the difference in effects from tobacco and cannabis was the amount of each that was smoked. Tobacco users typically smoked 10–20 cigarettes daily, some even more. Cannabis smokers, on average, smoked only two to three times a month, so the average exposure to cannabis was much lower than for tobacco. People experiment with cannabis in their late teens and 20s, and some consume relatively low levels for years. Although heavy exposure to cannabis might damage the lungs, reliable estimates of the effects of heavy use were not available in the 2012 study, as heavy users were relatively rare in the study population.
In the current analysis, we used data from UK Biobank (UKB) to assess the effect of cannabis on coronavirus disease (COVID-19) infection and to determine whether cannabis lung damage might facilitate COVID-19 infection in formerly heavy users.
The UKB is a large prospective observational study comprising about 500,000 men and women (N = 229,134 men, N = 273,402 women), more than 90% White, aged 40–69 years at enrollment. Participants were recruited from across 22 centers located throughout England, Wales, and Scotland, between 2006 and 2010, and continue to be longitudinally followed for capture of subsequent health events.2 This methodology is like that of the Framingham Heart Study,3 with the exception that the UKB program collects postmortem samples, which Framingham did not.
Our UKB application was approved as UKB project 57,245 (S.L. and P.H.R.).
Doctor-diagnosed chronic obstructive pulmonary disease (COPD) is from UKB data field 22,130. At enrollment, the subject was asked on a touchscreen, “Has a doctor ever told you that you have had any of the conditions below?” COPD was one of the options listed.
The subject was asked, “Have you taken cannabis (marijuana, grass, hash, ganja, blow, draw, skunk, weed, spliff, dope), even if it was a long time ago?” If the answer was “yes,” cannabis use was recorded in the UKB data field 20,454, maximum frequency of taking cannabis, question asked: “Considering when you were taking cannabis most regularly, how often did you take it?” Answers were 1 = Less than once a month, 2 = Once a month or more, but not every week, 3 = Once a week or more, but not every day, and 4 = Every day. Subject was then asked (UKB data field 20455) “About how old were you when you last had cannabis?”
All UKB subjects who had cannabis-use data, COVID-19 test data, and COPD data were included in the study.
Electronic linkage between UKB records and National Health Service COVID-19 laboratory test results in England were available from March 16 to April 26, 2020, including the peak of daily COVID-19 laboratory-confirmed cases in the current outbreak. During this period, testing of older groups was largely restricted to hospital inpatients with clinical signs of infection, so test positivity is considered a good marker of severe COVID-19.4
Data processing was performed on Minerva, a Linux mainframe with Centos 7.6, at the Icahn School of Medicine at Mount Sinai. We used the UKB Data Parser (ukbb parser), a python-based package that allows easy interfacing with the large UKB data set.5
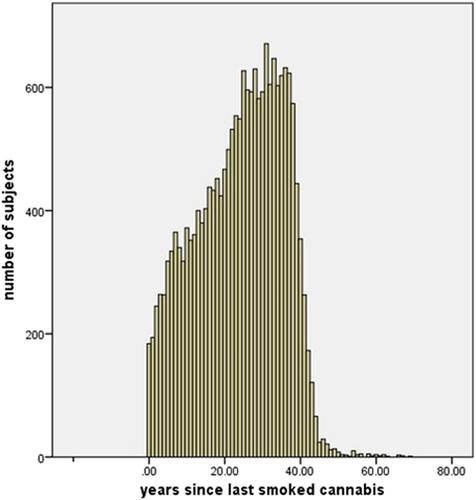
Mean age of subjects was 57 ± 8.1 (mean ± SD). Fifty-four percent were women and 46% were men. Ninety-eight percent were White British. Subjects had not smoked cannabis for 24 ± 11 years (Figure 1).
Cannabis maximum use versus COPD incidence in 20,996 subjects is shown in Table 1. Increasing cannabis use was associated with increased COPD prevalence (p = 0.011, Fisher's exact test, two tailed).
COVID-19 test result versus ever-taking cannabis is shown in Table 2. Increased cannabis use was associated with increased COVID-19 test positivity (p = 0.026, Fisher's exact test, two tailed).
Table 3 shows logistic regression, COVID-19 test result, dependent variable, ever-taking cannabis, pack-years smoking, and independent variables. The effects of cannabis and pack-years smoking on COVID-19 test result were significant and independent.
Tobacco smoking increases the risk of lung infections, possibly including COVID-19. Smoking impairs the immune system and almost doubles the risk of tuberculosis. Smoking affects macrophages and cytokine response, and therefore the ability to contain infection. The risk for pneumococcal, legionella, and mycoplasma pneumonia infection is about three to five times higher in smokers.6 In one study, current smokers were more likely to report symptoms, suggesting a diagnosis of COVID-19.7
The effects of smoking cannabis are difficult to assess accurately and to distinguish from the effects of tobacco; nevertheless, cannabis use may cause severe lung damage. Cannabis smoke affects the lungs similarly to tobacco smoke, causing symptoms such as increased cough, sputum, and hyperinflation. Cannabis can produce serious lung diseases with increasing years of use. Cannabis may weaken the immune system, leading to pneumonia. Smoking cannabis has been linked to symptoms of chronic bronchitis. Heavy use of cannabis can result in airway obstruction8 and worse COVID-19 outcome.9 Yet, cannabis use might reduce lung inflammation and inhibit viral replication10 in Covid-19 infections, leading to a better outcome in some cases.11, 12
As noted above, we found that the effects of cannabis and pack-years smoking on COVID-19 test result were significant and independent (Table 3). This suggests that the damaging effects of cannabis and smoking on the lung are additive, even though cannabis had not been smoked for a decade or more.
Our study has weaknesses. COVID-19-positive test results were related to cannabis use (Table 2). However, we did not have data relating the frequency of cannabis use to susceptibility COVID-19. In the logistic regression (Table 3), more independent variables would be worthwhile. Moreover, the high incidence of Caucasian subjects might influence the results.
It is never too late to quit smoking tobacco. As soon as a tobacco smoker quits, his chances are diminished of getting cancer and other diseases.13 Our findings imply that cannabis may be similar. Fifteen years after quitting tobacco, risk of coronary heart disease is close to that of a nonsmoker.14 Unlike the heart, the lung does not forget the insult from inhaled tobacco or cannabis, even many years later, but after quitting the lung damage may not further increase.
Changes in cannabis policies across states legalizing it for medical and recreational use suggest that cannabis is winning increased acceptance in our society. Thus, people must understand what is known about the adverse health effects of cannabis.15 As cannabis use becomes more widespread, no doubt more adverse effects will come to light.
Steven Lehrer and Peter H. Rheinstein contributed equally to this study.
The authors declare no conflict of interest.
UK Biobank has approval from the Northwest Multi-center Research Ethics Committee (MREC), which covers the United Kingdom. It also sought the approval in England and Wales from the Patient Information Advisory Group (PIAG) for gaining access to information that would allow it to invite people to participate. PIAG has since been replaced by the National Information Governance Board for Health & Social Care (NIGB). In Scotland, UK Biobank has approval from the Community Health Index Advisory Group (CHIAG).
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


