Padeepa Perera, Ronan O'Donnabhain, Timothy Fazio, Douglas Johnson, Peter Lange
{"title":"错过的治疗机会?SGLT-2抑制剂在普通内科心力衰竭患者中的应用:对三级医疗服务机构入院情况的回顾性审计","authors":"Padeepa Perera, Ronan O'Donnabhain, Timothy Fazio, Douglas Johnson, Peter Lange","doi":"10.1177/11795468221133607","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Sodium-glucose co-transporter-2 inhibitors (SGLT2-I's) are novel oral hypoglycaemic agents, with proven decreased MACE and re-hospitalisation risk in type 2 diabetic patients with concomitant heart failure. This study aimed to assess the current practice in the use of SGLT2-I's in general medical units at a large metropolitan health service.</p><p><strong>Methods/results: </strong>A retrospective audit was conducted of patients admitted to general medicine over a 12 month period (between April 2018 and 2019). Inclusion criteria included decompensated heart failure of any aetiology and ejection fraction, and type 2 diabetes mellitus with an HbA1c ⩾ 7 within 6 months of the admission period. A total of 150 admissions fulfilled criteria. Baseline demographics and comorbidities identified an older, more comorbid population than reference trials. These included age (75% over 75 years), smoking history (46%), hypertension (83%), chronic kidney disease grade IV or V (26%), previous myocardial infarction (57%), stroke (18%), atrial fibrillation (55%) and known left ventricular ejection fraction < 50% (38%). Co-prescribed medications included ACE-I/ARB (53%), beta-blocker (67%), loop diuretic (87%), thiazide (7%), MRA (31%), insulin (57%), metformin (47%), sulphonylurea (31%), DPP-4 Inhibitor (21%), GLP-1 analogue (6%) and 15% of patients had an HbA1c > 10. There was a significant difference between patients in our study eligible for and prescribed metformin (66/111) compared to SGLT-2 inhibitors (4/25) (<i>P</i> = .013). A total of 26 patients had readmissions within 28 days, of which one had been discharged on an SGLT2-I.</p><p><strong>Conclusion: </strong>The results of this study identified significant under prescribing of SGLT2-I's in eligible type 2 diabetic patients with heart failure admitted under general medicine.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":" ","pages":"11795468221133607"},"PeriodicalIF":3.3000,"publicationDate":"2022-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/2a/10.1177_11795468221133607.PMC9623351.pdf","citationCount":"1","resultStr":"{\"title\":\"'A Missed Therapeutic Opportunity? SGLT-2 Inhibitor Use in General Medicine Patients With Heart Failure: A Retrospective Audit of Admissions to a Tertiary Health Service'.\",\"authors\":\"Padeepa Perera, Ronan O'Donnabhain, Timothy Fazio, Douglas Johnson, Peter Lange\",\"doi\":\"10.1177/11795468221133607\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Sodium-glucose co-transporter-2 inhibitors (SGLT2-I's) are novel oral hypoglycaemic agents, with proven decreased MACE and re-hospitalisation risk in type 2 diabetic patients with concomitant heart failure. This study aimed to assess the current practice in the use of SGLT2-I's in general medical units at a large metropolitan health service.</p><p><strong>Methods/results: </strong>A retrospective audit was conducted of patients admitted to general medicine over a 12 month period (between April 2018 and 2019). Inclusion criteria included decompensated heart failure of any aetiology and ejection fraction, and type 2 diabetes mellitus with an HbA1c ⩾ 7 within 6 months of the admission period. A total of 150 admissions fulfilled criteria. Baseline demographics and comorbidities identified an older, more comorbid population than reference trials. These included age (75% over 75 years), smoking history (46%), hypertension (83%), chronic kidney disease grade IV or V (26%), previous myocardial infarction (57%), stroke (18%), atrial fibrillation (55%) and known left ventricular ejection fraction < 50% (38%). Co-prescribed medications included ACE-I/ARB (53%), beta-blocker (67%), loop diuretic (87%), thiazide (7%), MRA (31%), insulin (57%), metformin (47%), sulphonylurea (31%), DPP-4 Inhibitor (21%), GLP-1 analogue (6%) and 15% of patients had an HbA1c > 10. There was a significant difference between patients in our study eligible for and prescribed metformin (66/111) compared to SGLT-2 inhibitors (4/25) (<i>P</i> = .013). A total of 26 patients had readmissions within 28 days, of which one had been discharged on an SGLT2-I.</p><p><strong>Conclusion: </strong>The results of this study identified significant under prescribing of SGLT2-I's in eligible type 2 diabetic patients with heart failure admitted under general medicine.</p>\",\"PeriodicalId\":10419,\"journal\":{\"name\":\"Clinical Medicine Insights. Cardiology\",\"volume\":\" \",\"pages\":\"11795468221133607\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2022-10-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ef/2a/10.1177_11795468221133607.PMC9623351.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795468221133607\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468221133607","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
'A Missed Therapeutic Opportunity? SGLT-2 Inhibitor Use in General Medicine Patients With Heart Failure: A Retrospective Audit of Admissions to a Tertiary Health Service'.
Objective: Sodium-glucose co-transporter-2 inhibitors (SGLT2-I's) are novel oral hypoglycaemic agents, with proven decreased MACE and re-hospitalisation risk in type 2 diabetic patients with concomitant heart failure. This study aimed to assess the current practice in the use of SGLT2-I's in general medical units at a large metropolitan health service.
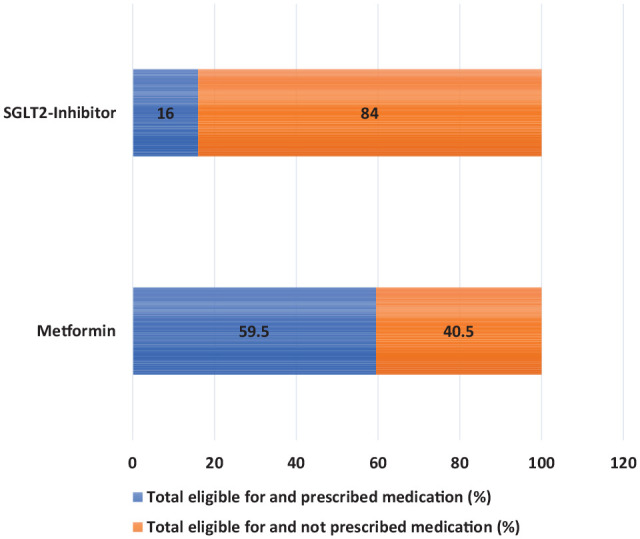
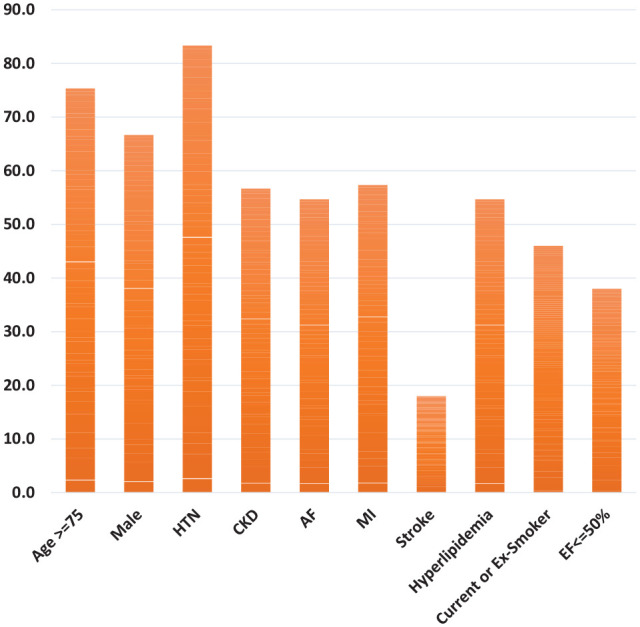
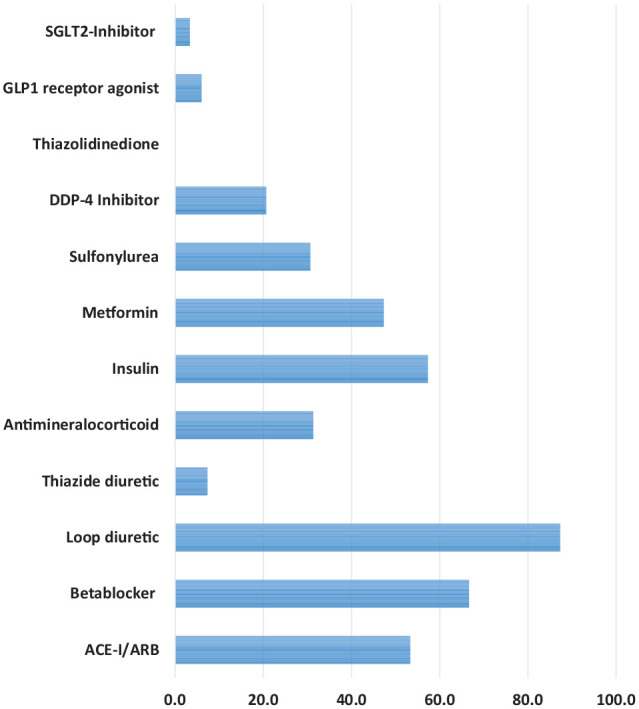
Methods/results: A retrospective audit was conducted of patients admitted to general medicine over a 12 month period (between April 2018 and 2019). Inclusion criteria included decompensated heart failure of any aetiology and ejection fraction, and type 2 diabetes mellitus with an HbA1c ⩾ 7 within 6 months of the admission period. A total of 150 admissions fulfilled criteria. Baseline demographics and comorbidities identified an older, more comorbid population than reference trials. These included age (75% over 75 years), smoking history (46%), hypertension (83%), chronic kidney disease grade IV or V (26%), previous myocardial infarction (57%), stroke (18%), atrial fibrillation (55%) and known left ventricular ejection fraction < 50% (38%). Co-prescribed medications included ACE-I/ARB (53%), beta-blocker (67%), loop diuretic (87%), thiazide (7%), MRA (31%), insulin (57%), metformin (47%), sulphonylurea (31%), DPP-4 Inhibitor (21%), GLP-1 analogue (6%) and 15% of patients had an HbA1c > 10. There was a significant difference between patients in our study eligible for and prescribed metformin (66/111) compared to SGLT-2 inhibitors (4/25) (P = .013). A total of 26 patients had readmissions within 28 days, of which one had been discharged on an SGLT2-I.
Conclusion: The results of this study identified significant under prescribing of SGLT2-I's in eligible type 2 diabetic patients with heart failure admitted under general medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


