Benjamin Cosway, Jonathan Fussey, Dae Kim, James Wykes, Michael Elliott, Joel Smith
{"title":"散发性甲状腺髓样癌:预测复发的临床病理和突变特征的系统回顾和荟萃分析。","authors":"Benjamin Cosway, Jonathan Fussey, Dae Kim, James Wykes, Michael Elliott, Joel Smith","doi":"10.1186/s13044-022-00130-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Sporadic medullary thyroid cancer accounts for 75% of all medullary thyroid cancers and presents at a more advanced disease stage than its hereditary counterparts. Yet there is little evidence to support risk stratification of patients according to risk of recurrence.</p><p><strong>Methods: </strong>A systematic review and meta-analysis was performed investigating clinical and pathological factors that are associated with recurrent disease in patients with medullary thyroid cancer.</p><p><strong>Results: </strong>10 studies totalling 458 patients were included in the meta-analyses. T3 and T4 disease (OR 9.33 (95% CI 2.5 - 34.82) p = 0.0009.), AJCC stage III and IV disease (OR 13.34 (95% CI 2.9 - 60.3) p = 0.0008) and the presence of nodal disease (OR 7.28 (95% CI 7.2-43.3) p = 0.03) were all associated with recurrent disease. RET mutations (OR 0.08 (95% CI -0.03-0.19) p = 0.17) and RET 918 T mutations (OR 1.77 (95% CI 0.804.0) P = 0.17) were not associated with disease recurrence. It was not possible to pool data with respect to extrathyroidal extension, extracapsular extension, peri-neural and lymphovascular invasion and RAS mutations.</p><p><strong>Conclusion: </strong>T3 and T4 disease, AJCC stage III and IV disease and the presence of nodal disease are associated with recurrent disease. The heterogeneous reporting of recurrence and the lack of individual patient data precludes larger scale meta-analyses. Future research in this area should involve collaboration to establish standardised definitions of disease recurrence.</p>","PeriodicalId":1,"journal":{"name":"Accounts of Chemical Research","volume":" ","pages":"12"},"PeriodicalIF":16.4000,"publicationDate":"2022-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9306201/pdf/","citationCount":"2","resultStr":"{\"title\":\"Sporadic medullary thyroid cancer: a systematic review and meta-analysis of clinico-pathological and mutational characteristics predicting recurrence.\",\"authors\":\"Benjamin Cosway, Jonathan Fussey, Dae Kim, James Wykes, Michael Elliott, Joel Smith\",\"doi\":\"10.1186/s13044-022-00130-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Sporadic medullary thyroid cancer accounts for 75% of all medullary thyroid cancers and presents at a more advanced disease stage than its hereditary counterparts. Yet there is little evidence to support risk stratification of patients according to risk of recurrence.</p><p><strong>Methods: </strong>A systematic review and meta-analysis was performed investigating clinical and pathological factors that are associated with recurrent disease in patients with medullary thyroid cancer.</p><p><strong>Results: </strong>10 studies totalling 458 patients were included in the meta-analyses. T3 and T4 disease (OR 9.33 (95% CI 2.5 - 34.82) p = 0.0009.), AJCC stage III and IV disease (OR 13.34 (95% CI 2.9 - 60.3) p = 0.0008) and the presence of nodal disease (OR 7.28 (95% CI 7.2-43.3) p = 0.03) were all associated with recurrent disease. RET mutations (OR 0.08 (95% CI -0.03-0.19) p = 0.17) and RET 918 T mutations (OR 1.77 (95% CI 0.804.0) P = 0.17) were not associated with disease recurrence. It was not possible to pool data with respect to extrathyroidal extension, extracapsular extension, peri-neural and lymphovascular invasion and RAS mutations.</p><p><strong>Conclusion: </strong>T3 and T4 disease, AJCC stage III and IV disease and the presence of nodal disease are associated with recurrent disease. The heterogeneous reporting of recurrence and the lack of individual patient data precludes larger scale meta-analyses. Future research in this area should involve collaboration to establish standardised definitions of disease recurrence.</p>\",\"PeriodicalId\":1,\"journal\":{\"name\":\"Accounts of Chemical Research\",\"volume\":\" \",\"pages\":\"12\"},\"PeriodicalIF\":16.4000,\"publicationDate\":\"2022-07-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9306201/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Accounts of Chemical Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13044-022-00130-8\",\"RegionNum\":1,\"RegionCategory\":\"化学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CHEMISTRY, MULTIDISCIPLINARY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Accounts of Chemical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-022-00130-8","RegionNum":1,"RegionCategory":"化学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CHEMISTRY, MULTIDISCIPLINARY","Score":null,"Total":0}
引用次数: 2
摘要
简介:散发性甲状腺髓样癌占所有甲状腺髓样癌的75%,与遗传性甲状腺髓样癌相比,散发性甲状腺髓样癌的病程更晚。然而,几乎没有证据支持根据复发风险对患者进行风险分层。方法:对甲状腺髓样癌患者疾病复发相关的临床和病理因素进行系统回顾和荟萃分析。结果:10项研究共纳入458例患者。T3和T4期疾病(OR 9.33 (95% CI 2.5 ~ 34.82) p = 0.0009)、AJCC III期和IV期疾病(OR 13.34 (95% CI 2.9 ~ 60.3) p = 0.0008)和淋巴结疾病的存在(OR 7.28 (95% CI 7.2 ~ 43.3) p = 0.03)均与疾病复发相关。RET突变(OR 0.08 (95% CI -0.03-0.19) p = 0.17)和RET 918t突变(OR 1.77 (95% CI 0.804.0) p = 0.17)与疾病复发无关。不可能汇集关于甲状腺外扩张、囊外扩张、神经和淋巴血管周围侵犯和RAS突变的数据。结论:T3和T4病变、AJCC III期和IV期病变及淋巴结病变的存在与疾病复发相关。复发报告的异质性和个体患者数据的缺乏妨碍了更大规模的荟萃分析。这一领域的未来研究应包括合作建立疾病复发的标准化定义。
Sporadic medullary thyroid cancer: a systematic review and meta-analysis of clinico-pathological and mutational characteristics predicting recurrence.
Introduction: Sporadic medullary thyroid cancer accounts for 75% of all medullary thyroid cancers and presents at a more advanced disease stage than its hereditary counterparts. Yet there is little evidence to support risk stratification of patients according to risk of recurrence.
Methods: A systematic review and meta-analysis was performed investigating clinical and pathological factors that are associated with recurrent disease in patients with medullary thyroid cancer.
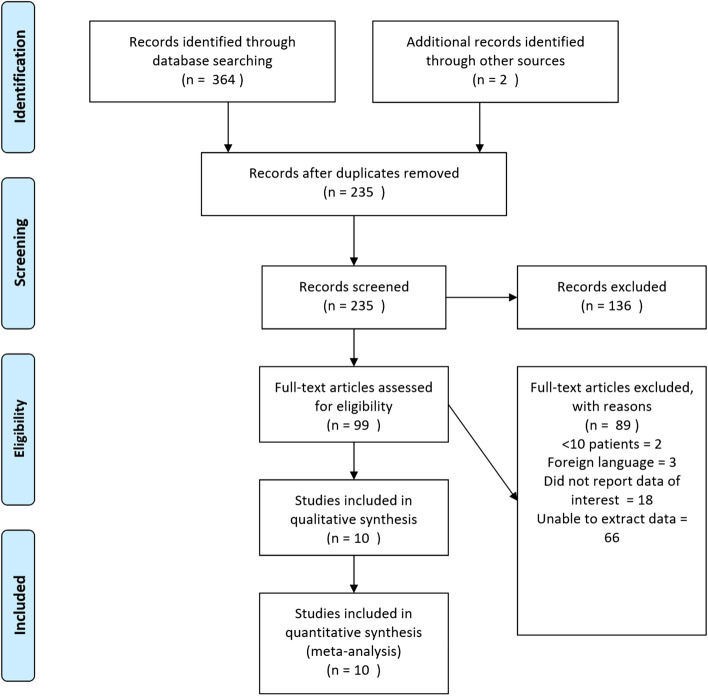
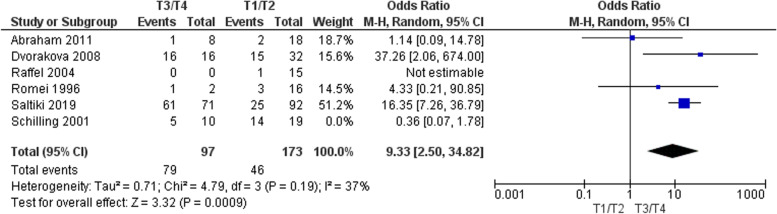
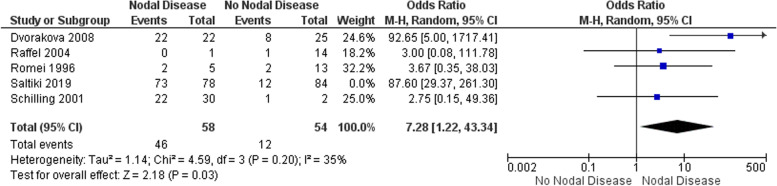
Results: 10 studies totalling 458 patients were included in the meta-analyses. T3 and T4 disease (OR 9.33 (95% CI 2.5 - 34.82) p = 0.0009.), AJCC stage III and IV disease (OR 13.34 (95% CI 2.9 - 60.3) p = 0.0008) and the presence of nodal disease (OR 7.28 (95% CI 7.2-43.3) p = 0.03) were all associated with recurrent disease. RET mutations (OR 0.08 (95% CI -0.03-0.19) p = 0.17) and RET 918 T mutations (OR 1.77 (95% CI 0.804.0) P = 0.17) were not associated with disease recurrence. It was not possible to pool data with respect to extrathyroidal extension, extracapsular extension, peri-neural and lymphovascular invasion and RAS mutations.
Conclusion: T3 and T4 disease, AJCC stage III and IV disease and the presence of nodal disease are associated with recurrent disease. The heterogeneous reporting of recurrence and the lack of individual patient data precludes larger scale meta-analyses. Future research in this area should involve collaboration to establish standardised definitions of disease recurrence.
期刊介绍:
Accounts of Chemical Research presents short, concise and critical articles offering easy-to-read overviews of basic research and applications in all areas of chemistry and biochemistry. These short reviews focus on research from the author’s own laboratory and are designed to teach the reader about a research project. In addition, Accounts of Chemical Research publishes commentaries that give an informed opinion on a current research problem. Special Issues online are devoted to a single topic of unusual activity and significance.
Accounts of Chemical Research replaces the traditional article abstract with an article "Conspectus." These entries synopsize the research affording the reader a closer look at the content and significance of an article. Through this provision of a more detailed description of the article contents, the Conspectus enhances the article's discoverability by search engines and the exposure for the research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


