{"title":"接受再灌注治疗的急性缺血性脑卒中患者血小板-淋巴细胞比值的预后作用:一项 Meta 分析。","authors":"Divyansh Sharma, Sonu M M Bhaskar","doi":"10.1177/11795735221110373","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Both inflammation and thrombotic/hemostatic mechanisms may play a role in acute ischemic stroke (AIS) pathogenesis, and a biomarker, such as the platelet-to-lymphocyte ratio (PLR), considering both mechanisms may be of clinical utility.</p><p><strong>Objectives: </strong>This meta-analysis sought to examine the effect of PLR on functional outcomes, early neurological changes, bleeding complications, mortality, and adverse outcomes in AIS patients treated with reperfusion therapy (RT).</p><p><strong>Design: </strong>Systematic Review and Meta-Analysis.</p><p><strong>Data sources and methods: </strong>Individual studies were retrieved from the PubMed/Medline, EMBASE and Cochrane databases. References thereof were also consulted. Data were extracted using a standardised data sheet, and systematic reviews and meta-analyses on the association of admission (pre-RT) or delayed (post-RT) PLR with defined clinical and safety outcomes were conducted. In the case of multiple delayed PLR timepoints, the timepoint closest to 24 hours was selected.</p><p><strong>Results: </strong>Eighteen studies (n=4878) were identified for the systematic review, of which 14 (n=4413) were included in the meta-analyses. PLR collected at admission was significantly negatively associated with 90-day good functional outcomes (SMD=-.32; 95% CI = -.58 to -.05; P=.020; z=-2.328), as was PLR collected at delayed timepoints (SMD=-.43; 95% CI = -.54 to -.32; P<.0001; z=-7.454). PLR at delayed timepoints was also significantly negatively associated with ENI (SMD=-.18; 95% CI = -.29 to -.08; P=.001. Conversely, the study suggested that a higher PLR at delayed timepoints may be associated with radiological bleeding and mortality. The results varied based on the type of RT administered.</p><p><strong>Conclusions: </strong>A higher PLR is associated with worse outcomes after stroke in terms of morbidity, mortality, and safety outcomes after stroke.</p>","PeriodicalId":15218,"journal":{"name":"Journal of Central Nervous System Disease","volume":null,"pages":null},"PeriodicalIF":2.6000,"publicationDate":"2022-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/52/c7/10.1177_11795735221110373.PMC9290168.pdf","citationCount":"0","resultStr":"{\"title\":\"Prognostic Role of the Platelet-Lymphocyte Ratio in Acute Ischemic Stroke Patients Undergoing Reperfusion Therapy: A Meta-Analysis.\",\"authors\":\"Divyansh Sharma, Sonu M M Bhaskar\",\"doi\":\"10.1177/11795735221110373\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Both inflammation and thrombotic/hemostatic mechanisms may play a role in acute ischemic stroke (AIS) pathogenesis, and a biomarker, such as the platelet-to-lymphocyte ratio (PLR), considering both mechanisms may be of clinical utility.</p><p><strong>Objectives: </strong>This meta-analysis sought to examine the effect of PLR on functional outcomes, early neurological changes, bleeding complications, mortality, and adverse outcomes in AIS patients treated with reperfusion therapy (RT).</p><p><strong>Design: </strong>Systematic Review and Meta-Analysis.</p><p><strong>Data sources and methods: </strong>Individual studies were retrieved from the PubMed/Medline, EMBASE and Cochrane databases. References thereof were also consulted. Data were extracted using a standardised data sheet, and systematic reviews and meta-analyses on the association of admission (pre-RT) or delayed (post-RT) PLR with defined clinical and safety outcomes were conducted. In the case of multiple delayed PLR timepoints, the timepoint closest to 24 hours was selected.</p><p><strong>Results: </strong>Eighteen studies (n=4878) were identified for the systematic review, of which 14 (n=4413) were included in the meta-analyses. PLR collected at admission was significantly negatively associated with 90-day good functional outcomes (SMD=-.32; 95% CI = -.58 to -.05; P=.020; z=-2.328), as was PLR collected at delayed timepoints (SMD=-.43; 95% CI = -.54 to -.32; P<.0001; z=-7.454). PLR at delayed timepoints was also significantly negatively associated with ENI (SMD=-.18; 95% CI = -.29 to -.08; P=.001. Conversely, the study suggested that a higher PLR at delayed timepoints may be associated with radiological bleeding and mortality. The results varied based on the type of RT administered.</p><p><strong>Conclusions: </strong>A higher PLR is associated with worse outcomes after stroke in terms of morbidity, mortality, and safety outcomes after stroke.</p>\",\"PeriodicalId\":15218,\"journal\":{\"name\":\"Journal of Central Nervous System Disease\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2022-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/52/c7/10.1177_11795735221110373.PMC9290168.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Central Nervous System Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795735221110373\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Central Nervous System Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795735221110373","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:炎症和血栓/止血机制都可能在急性缺血性卒中(AIS)发病机制中发挥作用,考虑这两种机制的生物标志物(如血小板与淋巴细胞比值(PLR))可能具有临床实用性:这项荟萃分析旨在研究 PLR 对接受再灌注疗法(RT)治疗的 AIS 患者的功能预后、早期神经系统变化、出血并发症、死亡率和不良预后的影响:数据来源和方法:从 PubMed/Medline、EMBASE 和 Cochrane 数据库中检索各项研究。此外,还查阅了相关参考文献。使用标准化数据表提取数据,并就入院(RT 前)或延迟(RT 后)PLR 与定义的临床和安全性结果的相关性进行系统综述和荟萃分析。如果存在多个延迟 PLR 时间点,则选择最接近 24 小时的时间点:系统综述确定了 18 项研究(n=4878),其中 14 项研究(n=4413)被纳入荟萃分析。入院时收集的PLR与90天良好功能预后呈显著负相关(SMD=-.32;95% CI = -.58 to -.05;P=.020;z=-2.328),延迟时间点收集的PLR也是如此(SMD=-.43;95% CI = -.54 to -.32;PC结论:就发病率、死亡率和安全性而言,较高的 PLR 与中风后较差的预后相关。
Prognostic Role of the Platelet-Lymphocyte Ratio in Acute Ischemic Stroke Patients Undergoing Reperfusion Therapy: A Meta-Analysis.
Background: Both inflammation and thrombotic/hemostatic mechanisms may play a role in acute ischemic stroke (AIS) pathogenesis, and a biomarker, such as the platelet-to-lymphocyte ratio (PLR), considering both mechanisms may be of clinical utility.
Objectives: This meta-analysis sought to examine the effect of PLR on functional outcomes, early neurological changes, bleeding complications, mortality, and adverse outcomes in AIS patients treated with reperfusion therapy (RT).
Design: Systematic Review and Meta-Analysis.
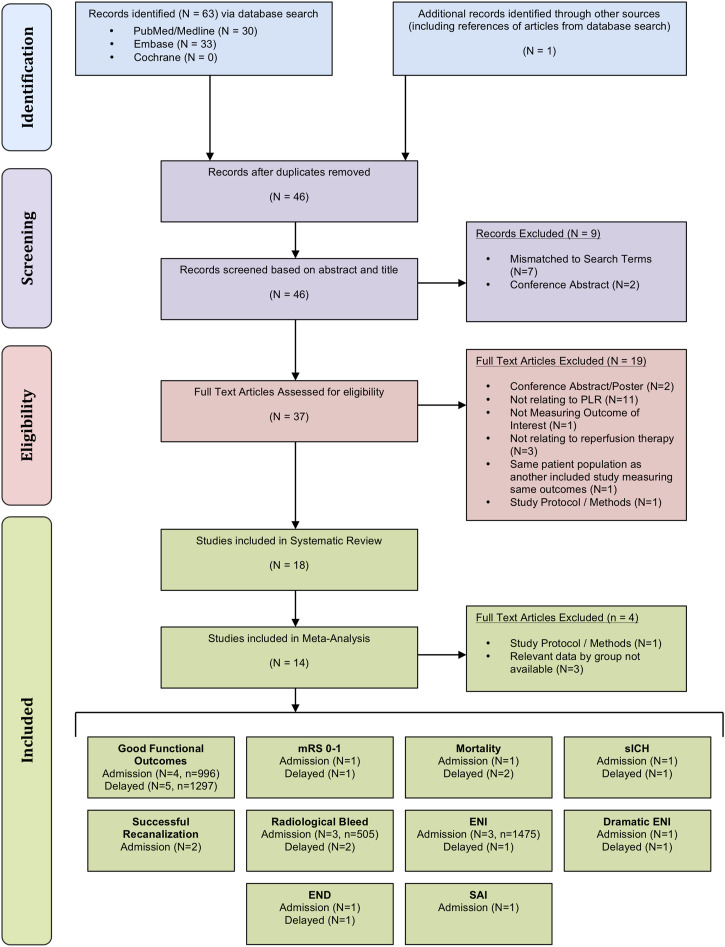
Data sources and methods: Individual studies were retrieved from the PubMed/Medline, EMBASE and Cochrane databases. References thereof were also consulted. Data were extracted using a standardised data sheet, and systematic reviews and meta-analyses on the association of admission (pre-RT) or delayed (post-RT) PLR with defined clinical and safety outcomes were conducted. In the case of multiple delayed PLR timepoints, the timepoint closest to 24 hours was selected.
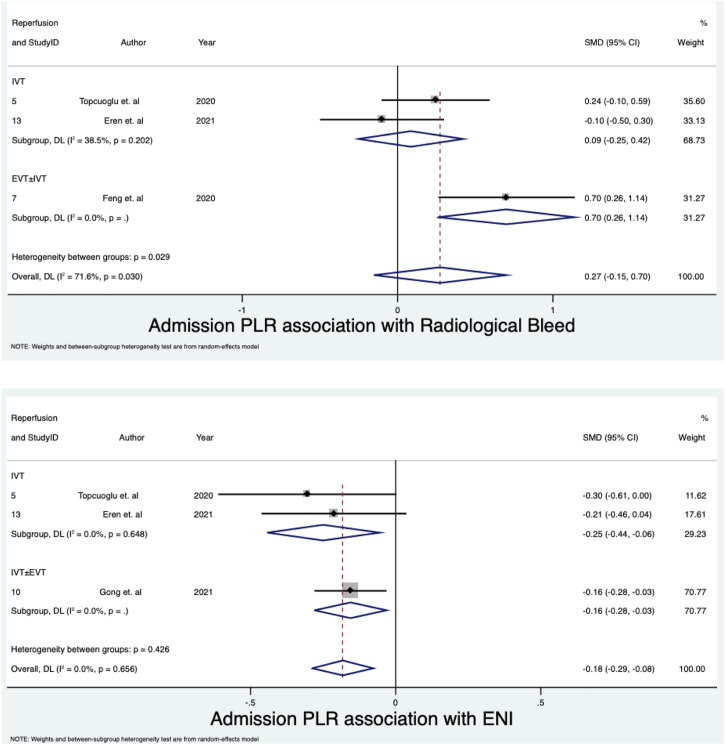
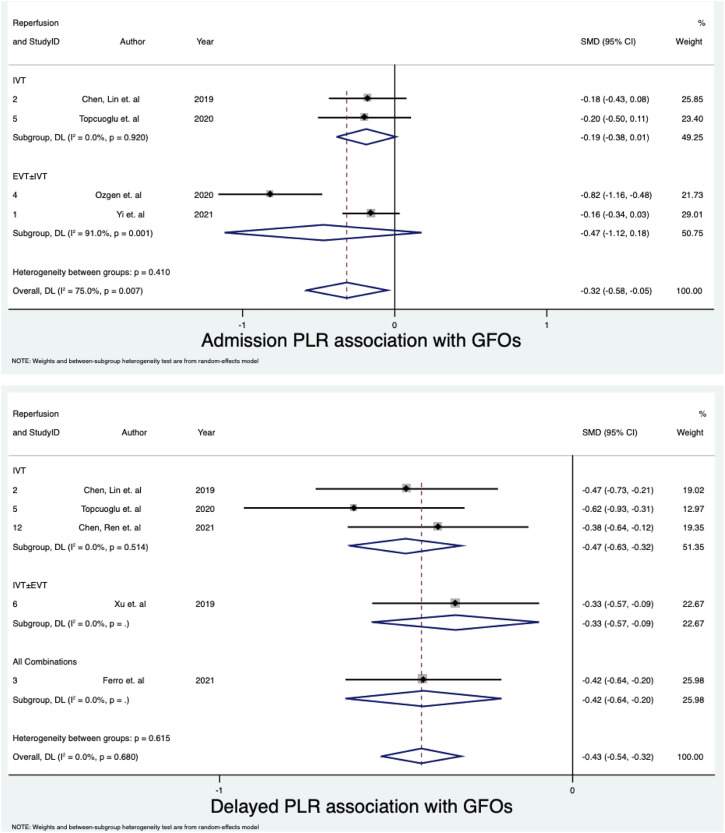
Results: Eighteen studies (n=4878) were identified for the systematic review, of which 14 (n=4413) were included in the meta-analyses. PLR collected at admission was significantly negatively associated with 90-day good functional outcomes (SMD=-.32; 95% CI = -.58 to -.05; P=.020; z=-2.328), as was PLR collected at delayed timepoints (SMD=-.43; 95% CI = -.54 to -.32; P<.0001; z=-7.454). PLR at delayed timepoints was also significantly negatively associated with ENI (SMD=-.18; 95% CI = -.29 to -.08; P=.001. Conversely, the study suggested that a higher PLR at delayed timepoints may be associated with radiological bleeding and mortality. The results varied based on the type of RT administered.
Conclusions: A higher PLR is associated with worse outcomes after stroke in terms of morbidity, mortality, and safety outcomes after stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


