Timothy McCann, Michael Fatuyi, Neha Patel, Deepali B Sharath, Anar S Patel
{"title":"耐甲氧西林金黄色葡萄球菌血流感染患者既往房颤与较高死亡率相关:全国住院患者样本分析","authors":"Timothy McCann, Michael Fatuyi, Neha Patel, Deepali B Sharath, Anar S Patel","doi":"10.1155/2022/8965888","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of this study was to investigate the prevalence of preexisting atrial fibrillation (AF) in patients with MRSA-BSI during a three-year period and the impact of preexisting AF on MRSA-BSI outcomes.</p><p><strong>Methods: </strong>This was a retrospective analysis performed using the National Inpatient Sample (NIS) over a three-year period (2016, 2017, 2018) for patients with MRSA-BSI as a principal diagnosis with and without preexisting AF. The primary outcome was mortality with secondary outcomes of acute coronary syndrome, cardiac arrest, cardiogenic shock, endocarditis, respiratory failure, acute kidney injury, length of stay, hospital cost, and patient charge. A univariate and multivariable logistic regression analysis estimated clinical outcomes.</p><p><strong>Results: </strong>Preexisting AF in patients with MRSA-BSI significantly increased the primary outcome of the study, mortality (1.67% vs. 0.66%, <i>p</i>=0.030) with an adjusted odds ratio (AOR) of 1.98 (95% CI, 1.1-3.7). Secondary outcomes showed increased likelihood of cardiac arrest with MRSA-BSI and AF (0.48% vs. 0.2%, <i>p</i>=0.025) with an AOR 3.59 (CI 1.18-11.0), ACS (3.44% vs. 1.21%, <i>p</i>=0.008) with an AOR of 1.81 (CI 1.16-2.80), respiratory failure (8.92% vs. 4.02%, <i>p</i>=0.045) with an AOR 1.39 (CI 1.01-1.91), prolonged LOS (6.4 vs. 5.4 days, <i>p</i>=0.0001), increased hospital cost ($13,374 vs. $11,401, <i>p</i>=0.0001), and increased overall patient charge ($50,091 vs. $43,018, <i>p</i>=0.0001). Secondary outcomes that showed statistical significance included ACS (1,497 (3.44%) vs. 113 (1.21%), <i>p</i>=0.008) with an AOR of 1.81 (CI 1.16-2.80), cardiac arrest (209 (0.48%) vs. 19 (0.2%), <i>p</i>=0.025) with an AOR 3.59 (CI 1.18-11.0), and respiratory failure (3,881 (8.92%) vs. 374 (4.02%), <i>p</i>=0.045 with an AOR 1.39 (CI 1.01-1.91).</p><p><strong>Conclusions: </strong>Preexisting AF is a significant risk factor for mortality in patients admitted for MRSA-BSI and increases risk for cardiac arrest, respiratory failure, and ACS. Considerations should focus on early treatment and source control, especially with AF given the mortality risk, increased hospitalization cost, and prolonged LOS.</p>","PeriodicalId":39128,"journal":{"name":"Interdisciplinary Perspectives on Infectious Diseases","volume":" ","pages":"8965888"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9325627/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preexisting Atrial Fibrillation Associated with Higher Mortality in Patients with Methicillin-Resistant <i>Staphylococcus aureus</i> Bloodstream Infections: Analysis of the National Inpatient Sample.\",\"authors\":\"Timothy McCann, Michael Fatuyi, Neha Patel, Deepali B Sharath, Anar S Patel\",\"doi\":\"10.1155/2022/8965888\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The purpose of this study was to investigate the prevalence of preexisting atrial fibrillation (AF) in patients with MRSA-BSI during a three-year period and the impact of preexisting AF on MRSA-BSI outcomes.</p><p><strong>Methods: </strong>This was a retrospective analysis performed using the National Inpatient Sample (NIS) over a three-year period (2016, 2017, 2018) for patients with MRSA-BSI as a principal diagnosis with and without preexisting AF. The primary outcome was mortality with secondary outcomes of acute coronary syndrome, cardiac arrest, cardiogenic shock, endocarditis, respiratory failure, acute kidney injury, length of stay, hospital cost, and patient charge. A univariate and multivariable logistic regression analysis estimated clinical outcomes.</p><p><strong>Results: </strong>Preexisting AF in patients with MRSA-BSI significantly increased the primary outcome of the study, mortality (1.67% vs. 0.66%, <i>p</i>=0.030) with an adjusted odds ratio (AOR) of 1.98 (95% CI, 1.1-3.7). Secondary outcomes showed increased likelihood of cardiac arrest with MRSA-BSI and AF (0.48% vs. 0.2%, <i>p</i>=0.025) with an AOR 3.59 (CI 1.18-11.0), ACS (3.44% vs. 1.21%, <i>p</i>=0.008) with an AOR of 1.81 (CI 1.16-2.80), respiratory failure (8.92% vs. 4.02%, <i>p</i>=0.045) with an AOR 1.39 (CI 1.01-1.91), prolonged LOS (6.4 vs. 5.4 days, <i>p</i>=0.0001), increased hospital cost ($13,374 vs. $11,401, <i>p</i>=0.0001), and increased overall patient charge ($50,091 vs. $43,018, <i>p</i>=0.0001). Secondary outcomes that showed statistical significance included ACS (1,497 (3.44%) vs. 113 (1.21%), <i>p</i>=0.008) with an AOR of 1.81 (CI 1.16-2.80), cardiac arrest (209 (0.48%) vs. 19 (0.2%), <i>p</i>=0.025) with an AOR 3.59 (CI 1.18-11.0), and respiratory failure (3,881 (8.92%) vs. 374 (4.02%), <i>p</i>=0.045 with an AOR 1.39 (CI 1.01-1.91).</p><p><strong>Conclusions: </strong>Preexisting AF is a significant risk factor for mortality in patients admitted for MRSA-BSI and increases risk for cardiac arrest, respiratory failure, and ACS. Considerations should focus on early treatment and source control, especially with AF given the mortality risk, increased hospitalization cost, and prolonged LOS.</p>\",\"PeriodicalId\":39128,\"journal\":{\"name\":\"Interdisciplinary Perspectives on Infectious Diseases\",\"volume\":\" \",\"pages\":\"8965888\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9325627/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interdisciplinary Perspectives on Infectious Diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/8965888\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Immunology and Microbiology\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary Perspectives on Infectious Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/8965888","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Immunology and Microbiology","Score":null,"Total":0}
Preexisting Atrial Fibrillation Associated with Higher Mortality in Patients with Methicillin-Resistant Staphylococcus aureus Bloodstream Infections: Analysis of the National Inpatient Sample.
Background: The purpose of this study was to investigate the prevalence of preexisting atrial fibrillation (AF) in patients with MRSA-BSI during a three-year period and the impact of preexisting AF on MRSA-BSI outcomes.
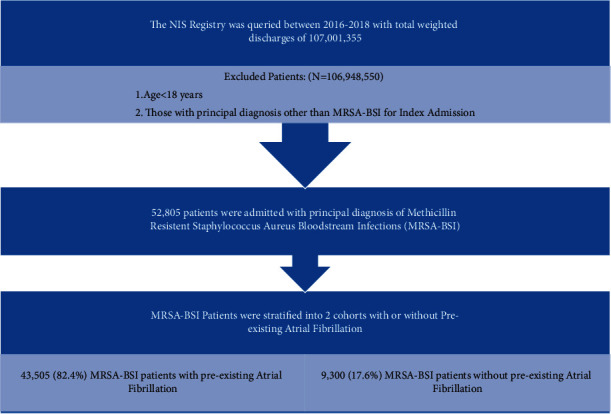
Methods: This was a retrospective analysis performed using the National Inpatient Sample (NIS) over a three-year period (2016, 2017, 2018) for patients with MRSA-BSI as a principal diagnosis with and without preexisting AF. The primary outcome was mortality with secondary outcomes of acute coronary syndrome, cardiac arrest, cardiogenic shock, endocarditis, respiratory failure, acute kidney injury, length of stay, hospital cost, and patient charge. A univariate and multivariable logistic regression analysis estimated clinical outcomes.
Results: Preexisting AF in patients with MRSA-BSI significantly increased the primary outcome of the study, mortality (1.67% vs. 0.66%, p=0.030) with an adjusted odds ratio (AOR) of 1.98 (95% CI, 1.1-3.7). Secondary outcomes showed increased likelihood of cardiac arrest with MRSA-BSI and AF (0.48% vs. 0.2%, p=0.025) with an AOR 3.59 (CI 1.18-11.0), ACS (3.44% vs. 1.21%, p=0.008) with an AOR of 1.81 (CI 1.16-2.80), respiratory failure (8.92% vs. 4.02%, p=0.045) with an AOR 1.39 (CI 1.01-1.91), prolonged LOS (6.4 vs. 5.4 days, p=0.0001), increased hospital cost ($13,374 vs. $11,401, p=0.0001), and increased overall patient charge ($50,091 vs. $43,018, p=0.0001). Secondary outcomes that showed statistical significance included ACS (1,497 (3.44%) vs. 113 (1.21%), p=0.008) with an AOR of 1.81 (CI 1.16-2.80), cardiac arrest (209 (0.48%) vs. 19 (0.2%), p=0.025) with an AOR 3.59 (CI 1.18-11.0), and respiratory failure (3,881 (8.92%) vs. 374 (4.02%), p=0.045 with an AOR 1.39 (CI 1.01-1.91).
Conclusions: Preexisting AF is a significant risk factor for mortality in patients admitted for MRSA-BSI and increases risk for cardiac arrest, respiratory failure, and ACS. Considerations should focus on early treatment and source control, especially with AF given the mortality risk, increased hospitalization cost, and prolonged LOS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


