Paul C Mullan, Christopher M Pruitt, Kelly A Levasseur, Charles G Macias, Raina Paul, Holly Depinet, Anh Thy H Nguyen, Elliot Melendez
{"title":"静脉输液率与儿童脓毒症的预后相关:一项多中心分析","authors":"Paul C Mullan, Christopher M Pruitt, Kelly A Levasseur, Charles G Macias, Raina Paul, Holly Depinet, Anh Thy H Nguyen, Elliot Melendez","doi":"10.2147/OAEM.S368442","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Pediatric sepsis guidelines recommend rapid intravenous fluid (IVF) bolus administration rates (BAR). Recent sepsis studies suggest that rapid BAR may be associated with increased morbidity. We aimed to describe the association between emergency department (ED) IVF BAR and clinical outcomes in pediatric sepsis.</p><p><strong>Patients and methods: </strong>Secondary post-hoc analysis of retrospective cohort data from 19 hospitals in the Pediatric Septic Shock Collaborative (PSSC) database. Patients with presumed septic shock were defined by severe sepsis/septic shock diagnostic codes, receipt of septic shock therapies, or floor-to-ICU transfers within 12 hours from ED admission for septic shock. Patients (2 months-21 years) with complete data on weight, antibiotic receipt, bolus timing, and bolus volumes were included. The primary outcome was 30-day mortality. Associations between BAR and mortality and secondary (intubation or non-invasive positive pressure ventilation = NIPPV) outcomes were assessed using unadjusted and adjusted logistic regression.</p><p><strong>Results: </strong>The PSSC database included 6731 patients; 3969 met inclusion and received a median ED volume of 40.2 mL/kg. Seventy-six (1.9%) patients died, 151 (3.8%) were intubated, and 235 (5.9%) had NIPPV administered. The median BAR was 25.7 mL/kg/hr. For each 20 mL/kg/hr increase in BAR, the adjusted odds ratio (aOR) for 30-day mortality [aOR = 1.11 (95% CI 1.01, 1.23)], intubation [aOR = 1.25 (95% CI 1.09, 1.44)], and NIPPV [aOR = 1.20 (95% CI 1.05, 1.38)] significantly increased.</p><p><strong>Conclusion: </strong>Faster ED IVF bolus administration rates in this pediatric sepsis database were associated with higher adjusted odds of death, intubation and NIPPV. Controlled trials are needed to determine if these associations are replicable.</p>","PeriodicalId":503614,"journal":{"name":"Open Access Emergency Medicine : OAEM","volume":" ","pages":"375-384"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/32/44/oaem-14-375.PMC9342868.pdf","citationCount":"2","resultStr":"{\"title\":\"Intravenous Fluid Bolus Rates Associated with Outcomes in Pediatric Sepsis: A Multi-Center Analysis.\",\"authors\":\"Paul C Mullan, Christopher M Pruitt, Kelly A Levasseur, Charles G Macias, Raina Paul, Holly Depinet, Anh Thy H Nguyen, Elliot Melendez\",\"doi\":\"10.2147/OAEM.S368442\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Pediatric sepsis guidelines recommend rapid intravenous fluid (IVF) bolus administration rates (BAR). Recent sepsis studies suggest that rapid BAR may be associated with increased morbidity. We aimed to describe the association between emergency department (ED) IVF BAR and clinical outcomes in pediatric sepsis.</p><p><strong>Patients and methods: </strong>Secondary post-hoc analysis of retrospective cohort data from 19 hospitals in the Pediatric Septic Shock Collaborative (PSSC) database. Patients with presumed septic shock were defined by severe sepsis/septic shock diagnostic codes, receipt of septic shock therapies, or floor-to-ICU transfers within 12 hours from ED admission for septic shock. Patients (2 months-21 years) with complete data on weight, antibiotic receipt, bolus timing, and bolus volumes were included. The primary outcome was 30-day mortality. Associations between BAR and mortality and secondary (intubation or non-invasive positive pressure ventilation = NIPPV) outcomes were assessed using unadjusted and adjusted logistic regression.</p><p><strong>Results: </strong>The PSSC database included 6731 patients; 3969 met inclusion and received a median ED volume of 40.2 mL/kg. Seventy-six (1.9%) patients died, 151 (3.8%) were intubated, and 235 (5.9%) had NIPPV administered. The median BAR was 25.7 mL/kg/hr. For each 20 mL/kg/hr increase in BAR, the adjusted odds ratio (aOR) for 30-day mortality [aOR = 1.11 (95% CI 1.01, 1.23)], intubation [aOR = 1.25 (95% CI 1.09, 1.44)], and NIPPV [aOR = 1.20 (95% CI 1.05, 1.38)] significantly increased.</p><p><strong>Conclusion: </strong>Faster ED IVF bolus administration rates in this pediatric sepsis database were associated with higher adjusted odds of death, intubation and NIPPV. Controlled trials are needed to determine if these associations are replicable.</p>\",\"PeriodicalId\":503614,\"journal\":{\"name\":\"Open Access Emergency Medicine : OAEM\",\"volume\":\" \",\"pages\":\"375-384\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/32/44/oaem-14-375.PMC9342868.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine : OAEM\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S368442\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine : OAEM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S368442","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
摘要
目的:儿科败血症指南推荐快速静脉输液(IVF)丸给药率(BAR)。最近的脓毒症研究表明,快速BAR可能与发病率增加有关。我们的目的是描述急诊科(ED) IVF BAR与儿科败血症临床结果之间的关系。患者和方法:对儿童感染性休克协作(PSSC)数据库中19家医院的回顾性队列数据进行二次事后分析。假定的脓毒性休克患者通过严重脓毒症/脓毒性休克诊断代码、接受脓毒性休克治疗或因脓毒性休克入院后12小时内转至icu进行定义。患者(2个月-21岁)具有完整的体重、抗生素使用、给药时间和给药量数据。主要终点为30天死亡率。BAR与死亡率和继发性(插管或无创正压通气= NIPPV)结果之间的关系采用未调整和调整的逻辑回归进行评估。结果:PSSC数据库包括6731例患者;3969例患者符合纳入标准,ED的中位容积为40.2 mL/kg。76例(1.9%)患者死亡,151例(3.8%)患者插管,235例(5.9%)患者给予NIPPV。中位BAR为25.7 mL/kg/hr。BAR每增加20 mL/kg/hr, 30天死亡率的调整优势比(aOR) [aOR = 1.11 (95% CI 1.01, 1.23)]、插管[aOR = 1.25 (95% CI 1.09, 1.44)]和NIPPV [aOR = 1.20 (95% CI 1.05, 1.38)]显著增加。结论:在这个儿童败血症数据库中,更快的ED IVF给药率与更高的调整后死亡、插管和NIPPV的几率相关。需要对照试验来确定这些关联是否可复制。
Intravenous Fluid Bolus Rates Associated with Outcomes in Pediatric Sepsis: A Multi-Center Analysis.
Purpose: Pediatric sepsis guidelines recommend rapid intravenous fluid (IVF) bolus administration rates (BAR). Recent sepsis studies suggest that rapid BAR may be associated with increased morbidity. We aimed to describe the association between emergency department (ED) IVF BAR and clinical outcomes in pediatric sepsis.
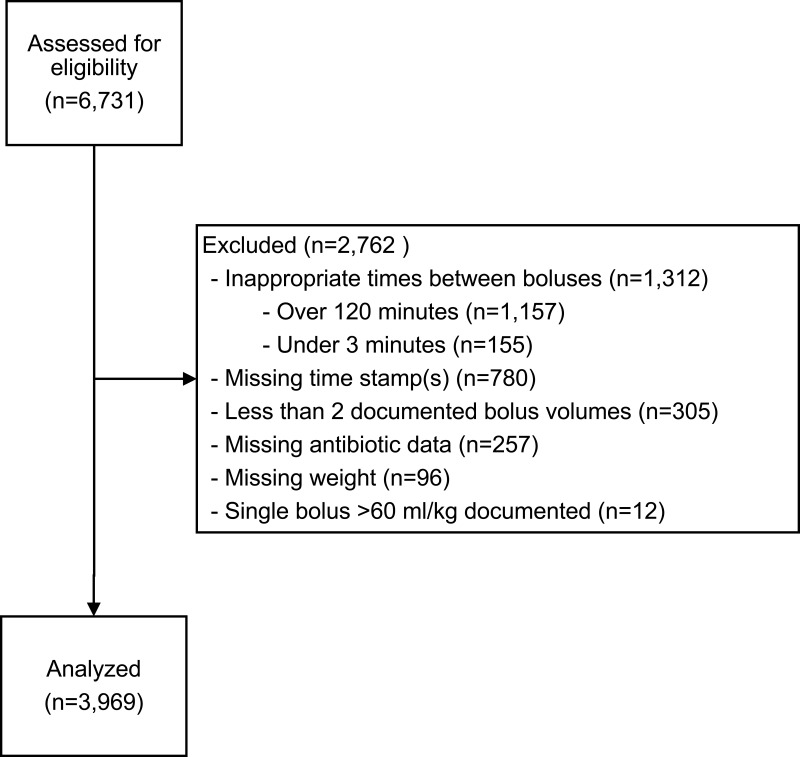
Patients and methods: Secondary post-hoc analysis of retrospective cohort data from 19 hospitals in the Pediatric Septic Shock Collaborative (PSSC) database. Patients with presumed septic shock were defined by severe sepsis/septic shock diagnostic codes, receipt of septic shock therapies, or floor-to-ICU transfers within 12 hours from ED admission for septic shock. Patients (2 months-21 years) with complete data on weight, antibiotic receipt, bolus timing, and bolus volumes were included. The primary outcome was 30-day mortality. Associations between BAR and mortality and secondary (intubation or non-invasive positive pressure ventilation = NIPPV) outcomes were assessed using unadjusted and adjusted logistic regression.
Results: The PSSC database included 6731 patients; 3969 met inclusion and received a median ED volume of 40.2 mL/kg. Seventy-six (1.9%) patients died, 151 (3.8%) were intubated, and 235 (5.9%) had NIPPV administered. The median BAR was 25.7 mL/kg/hr. For each 20 mL/kg/hr increase in BAR, the adjusted odds ratio (aOR) for 30-day mortality [aOR = 1.11 (95% CI 1.01, 1.23)], intubation [aOR = 1.25 (95% CI 1.09, 1.44)], and NIPPV [aOR = 1.20 (95% CI 1.05, 1.38)] significantly increased.
Conclusion: Faster ED IVF bolus administration rates in this pediatric sepsis database were associated with higher adjusted odds of death, intubation and NIPPV. Controlled trials are needed to determine if these associations are replicable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


