{"title":"心脏小组介入钙化左主干冠状动脉病变及危及左乳内动脉移植物。","authors":"Nobunari Tomura, Masashi Fujino, Yu Kataoka, Shuichi Yoneda, Hiroaki Sasaki, Teruo Noguchi","doi":"10.1155/2022/7712888","DOIUrl":null,"url":null,"abstract":"<p><p>It is sometimes difficult to identify the culprit lesion and treatment strategy in patients with acute coronary syndrome who have complex coronary lesions and jeopardized left internal mammary artery graft. This report describes a heart team approach for a non-ST-segment elevation myocardial infarction case with complex coronary vasculature. A 73-year-old man presented to the emergency department with crescendo angina. He had a history of total aortic arch replacement with concomitant coronary artery bypass graft using left internal mammary artery. Emergent coronary angiography demonstrated severe stenosis at left main trunk bifurcation caused by calcified nodule. While the bypass graft to left anterior descending coronary artery was patent, the proximal segment of left subclavian artery was occluded. Following the prompt discussion with our heart team, we performed percutaneous coronary intervention in the first step for treating the left main stenosis using rotational atherectomy into the unprotected left circumflex artery. After clinical recovery, stress myocardial scintigraphy identified the presence of anteroseptal ischemia, which indicated coronary subclavian steal syndrome due to left subclavian artery occlusion. Contrast-enhanced CT visualized that the occlusion originated from the anastomosis, suggesting the potential procedural risk of endovascular treatment by dilatation. Our heart team discussed again and decided to undergo axillo-axillary artery bypass surgery. He was discharged 8 days after the surgery without any sequelae. This is the rare case report of non-ST-segment elevation myocardial infarction who had similar condition to coronary subclavian steal syndrome after total aortic arch replacement. This case highlights the importance of a collaborative approach of the heart team to identify the best therapeutic strategy in a patient with complex coronary vasculature.</p>","PeriodicalId":51760,"journal":{"name":"Case Reports in Cardiology","volume":" ","pages":"7712888"},"PeriodicalIF":0.6000,"publicationDate":"2022-06-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9242785/pdf/","citationCount":"0","resultStr":"{\"title\":\"Heart Team Intervention for Calcified Left Main Coronary Disease and Jeopardized Left Internal Mammary Artery Graft.\",\"authors\":\"Nobunari Tomura, Masashi Fujino, Yu Kataoka, Shuichi Yoneda, Hiroaki Sasaki, Teruo Noguchi\",\"doi\":\"10.1155/2022/7712888\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>It is sometimes difficult to identify the culprit lesion and treatment strategy in patients with acute coronary syndrome who have complex coronary lesions and jeopardized left internal mammary artery graft. This report describes a heart team approach for a non-ST-segment elevation myocardial infarction case with complex coronary vasculature. A 73-year-old man presented to the emergency department with crescendo angina. He had a history of total aortic arch replacement with concomitant coronary artery bypass graft using left internal mammary artery. Emergent coronary angiography demonstrated severe stenosis at left main trunk bifurcation caused by calcified nodule. While the bypass graft to left anterior descending coronary artery was patent, the proximal segment of left subclavian artery was occluded. Following the prompt discussion with our heart team, we performed percutaneous coronary intervention in the first step for treating the left main stenosis using rotational atherectomy into the unprotected left circumflex artery. After clinical recovery, stress myocardial scintigraphy identified the presence of anteroseptal ischemia, which indicated coronary subclavian steal syndrome due to left subclavian artery occlusion. Contrast-enhanced CT visualized that the occlusion originated from the anastomosis, suggesting the potential procedural risk of endovascular treatment by dilatation. Our heart team discussed again and decided to undergo axillo-axillary artery bypass surgery. He was discharged 8 days after the surgery without any sequelae. This is the rare case report of non-ST-segment elevation myocardial infarction who had similar condition to coronary subclavian steal syndrome after total aortic arch replacement. This case highlights the importance of a collaborative approach of the heart team to identify the best therapeutic strategy in a patient with complex coronary vasculature.</p>\",\"PeriodicalId\":51760,\"journal\":{\"name\":\"Case Reports in Cardiology\",\"volume\":\" \",\"pages\":\"7712888\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2022-06-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9242785/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/7712888\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/7712888","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Heart Team Intervention for Calcified Left Main Coronary Disease and Jeopardized Left Internal Mammary Artery Graft.
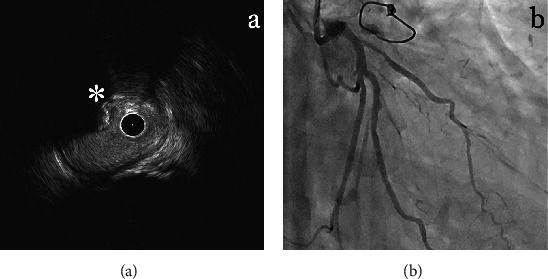
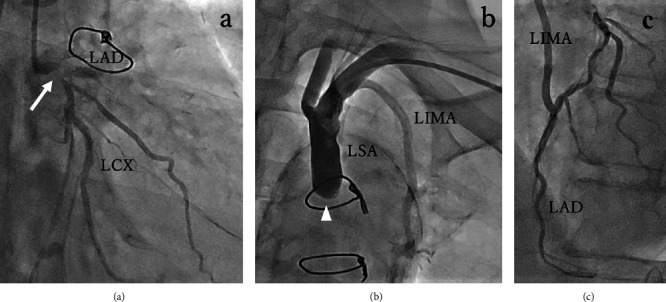
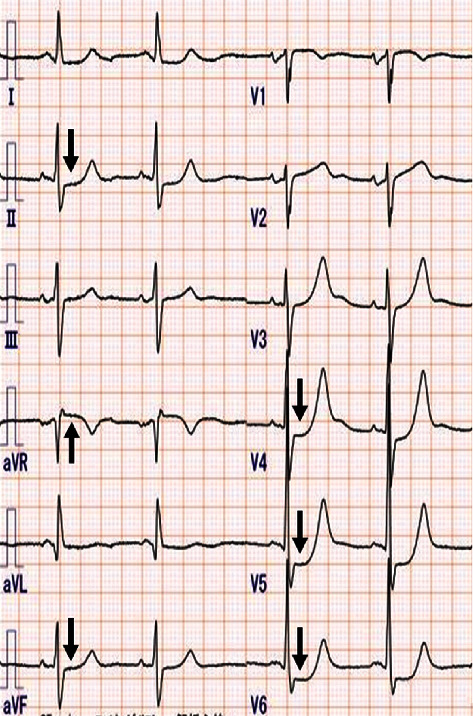
It is sometimes difficult to identify the culprit lesion and treatment strategy in patients with acute coronary syndrome who have complex coronary lesions and jeopardized left internal mammary artery graft. This report describes a heart team approach for a non-ST-segment elevation myocardial infarction case with complex coronary vasculature. A 73-year-old man presented to the emergency department with crescendo angina. He had a history of total aortic arch replacement with concomitant coronary artery bypass graft using left internal mammary artery. Emergent coronary angiography demonstrated severe stenosis at left main trunk bifurcation caused by calcified nodule. While the bypass graft to left anterior descending coronary artery was patent, the proximal segment of left subclavian artery was occluded. Following the prompt discussion with our heart team, we performed percutaneous coronary intervention in the first step for treating the left main stenosis using rotational atherectomy into the unprotected left circumflex artery. After clinical recovery, stress myocardial scintigraphy identified the presence of anteroseptal ischemia, which indicated coronary subclavian steal syndrome due to left subclavian artery occlusion. Contrast-enhanced CT visualized that the occlusion originated from the anastomosis, suggesting the potential procedural risk of endovascular treatment by dilatation. Our heart team discussed again and decided to undergo axillo-axillary artery bypass surgery. He was discharged 8 days after the surgery without any sequelae. This is the rare case report of non-ST-segment elevation myocardial infarction who had similar condition to coronary subclavian steal syndrome after total aortic arch replacement. This case highlights the importance of a collaborative approach of the heart team to identify the best therapeutic strategy in a patient with complex coronary vasculature.
期刊介绍:
Case Reports in Cardiology is a peer-reviewed, Open Access journal that publishes case reports and case series related to hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease and cardiomyopathy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


