James W Malcolmson, Rebecca K Hughes, Abhishek Joshi, Jackie Cooper, Alexander Breitenstein, Matthew Ginks, Steffen E Petersen, Saidi A Mohiddin, Mehul B Dhinoja
{"title":"中腔梗阻性肥厚性心肌病远端心室起搏的治疗效果。","authors":"James W Malcolmson, Rebecca K Hughes, Abhishek Joshi, Jackie Cooper, Alexander Breitenstein, Matthew Ginks, Steffen E Petersen, Saidi A Mohiddin, Mehul B Dhinoja","doi":"10.1177/17539447221108816","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hypertrophic cardiomyopathy (HCM) patients with left ventricular (LV) mid-cavity obstruction (LVMCO) often experience severe drug-refractory symptoms thought to be related to intraventricular obstruction. We tested whether ventricular pacing, guided by invasive haemodynamic assessment, reduced LVMCO and improved refractory symptoms.</p><p><strong>Methods: </strong>Between December 2008 and December 2017, 16 HCM patients with severe refractory symptoms and LVMCO underwent device implantation with haemodynamic pacing study to assess the effect on invasively defined LVMCO gradients. The effect on the gradient of atrioventricular (AV) synchronous pacing from sites including right ventricular (RV) apex and middle cardiac vein (MCV) was retrospectively assessed.</p><p><strong>Results: </strong>Invasive haemodynamic data were available in 14 of 16 patients. Mean pre-treatment intracavitary gradient was 77 ± 22 mmHg (in sinus rhythm) <i>versus</i> 21 ± 21 mmHg during pacing from optimal ventricular site (95% CI: -70.86 to -40.57, <i>p</i> < 0.0001). Optimal pacing site was distal MCV in 12/16 (86%), RV apex in 1/16 and via epicardial LV lead in 1/16. Pre-pacing Doppler-derived gradients were significantly higher than at follow-up (47 ± 15 <i>versus</i> 24 ± 16 mmHg, 95% CI: -37.19 to -13.73, <i>p</i> < 0.001). Median baseline NYHA class was 3, which had improved by ⩾1 NYHA class in 13 of 16 patients at 1-year post-procedure (<i>p</i> < 0.001). The mean follow-up duration was 4.6 ± 2.7 years with the following outcomes: 8/16 (50%) had continued symptomatic improvement, 4/16 had symptomatic decline and 4/16 died. Contributors to symptomatic decline included chronic atrial fibrillation (AF) (<i>n</i> = 5), phrenic nerve stimulation (<i>n</i> = 3) and ventricular ectopy (<i>n</i> = 1).</p><p><strong>Conclusion: </strong>In drug-refractory symptomatic LVMCO, distal ventricular pacing can reduce intracavitary obstruction and may provide long-term symptomatic relief in patients with limited treatment options. A haemodynamic pacing study is an effective strategy for identifying optimal pacing site and configuration.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":" ","pages":"17539447221108816"},"PeriodicalIF":2.2000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/80/10.1177_17539447221108816.PMC9350522.pdf","citationCount":"1","resultStr":"{\"title\":\"Therapeutic benefits of distal ventricular pacing in mid-cavity obstructive hypertrophic cardiomyopathy.\",\"authors\":\"James W Malcolmson, Rebecca K Hughes, Abhishek Joshi, Jackie Cooper, Alexander Breitenstein, Matthew Ginks, Steffen E Petersen, Saidi A Mohiddin, Mehul B Dhinoja\",\"doi\":\"10.1177/17539447221108816\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hypertrophic cardiomyopathy (HCM) patients with left ventricular (LV) mid-cavity obstruction (LVMCO) often experience severe drug-refractory symptoms thought to be related to intraventricular obstruction. We tested whether ventricular pacing, guided by invasive haemodynamic assessment, reduced LVMCO and improved refractory symptoms.</p><p><strong>Methods: </strong>Between December 2008 and December 2017, 16 HCM patients with severe refractory symptoms and LVMCO underwent device implantation with haemodynamic pacing study to assess the effect on invasively defined LVMCO gradients. The effect on the gradient of atrioventricular (AV) synchronous pacing from sites including right ventricular (RV) apex and middle cardiac vein (MCV) was retrospectively assessed.</p><p><strong>Results: </strong>Invasive haemodynamic data were available in 14 of 16 patients. Mean pre-treatment intracavitary gradient was 77 ± 22 mmHg (in sinus rhythm) <i>versus</i> 21 ± 21 mmHg during pacing from optimal ventricular site (95% CI: -70.86 to -40.57, <i>p</i> < 0.0001). Optimal pacing site was distal MCV in 12/16 (86%), RV apex in 1/16 and via epicardial LV lead in 1/16. Pre-pacing Doppler-derived gradients were significantly higher than at follow-up (47 ± 15 <i>versus</i> 24 ± 16 mmHg, 95% CI: -37.19 to -13.73, <i>p</i> < 0.001). Median baseline NYHA class was 3, which had improved by ⩾1 NYHA class in 13 of 16 patients at 1-year post-procedure (<i>p</i> < 0.001). The mean follow-up duration was 4.6 ± 2.7 years with the following outcomes: 8/16 (50%) had continued symptomatic improvement, 4/16 had symptomatic decline and 4/16 died. Contributors to symptomatic decline included chronic atrial fibrillation (AF) (<i>n</i> = 5), phrenic nerve stimulation (<i>n</i> = 3) and ventricular ectopy (<i>n</i> = 1).</p><p><strong>Conclusion: </strong>In drug-refractory symptomatic LVMCO, distal ventricular pacing can reduce intracavitary obstruction and may provide long-term symptomatic relief in patients with limited treatment options. A haemodynamic pacing study is an effective strategy for identifying optimal pacing site and configuration.</p>\",\"PeriodicalId\":23035,\"journal\":{\"name\":\"Therapeutic Advances in Cardiovascular Disease\",\"volume\":\" \",\"pages\":\"17539447221108816\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/42/80/10.1177_17539447221108816.PMC9350522.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/17539447221108816\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17539447221108816","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
摘要
肥厚性心肌病(HCM)合并左心室(LV)中腔梗阻(LVMCO)的患者通常会出现严重的药物难治性症状,这些症状被认为与室内梗阻有关。我们测试了在有创血流动力学评估指导下的心室起搏是否能降低lvco并改善难治性症状。方法:2008年12月至2017年12月,16例伴有严重难治性症状和lvco的HCM患者接受了血液动力学起搏装置植入研究,以评估有创定义的lvco梯度的影响。回顾性评价右心室(RV)心尖和心中静脉(MCV)等部位对房室(AV)同步起搏梯度的影响。结果:16例患者中有14例获得有创血流动力学数据。治疗前平均腔内梯度为77±22 mmHg(窦性心律),而起搏时为21±21 mmHg (95% CI: -70.86至-40.57,p对24±16 mmHg, 95% CI: -37.19至-13.73,p p n = 5),膈神经刺激(n = 3)和心室异位(n = 1)。结论:对于难治性症状性lvco,远端心室起搏可以减少腔内阻塞,并可能为治疗选择有限的患者提供长期症状缓解。血流动力学起搏研究是确定最佳起搏部位和配置的有效策略。
Therapeutic benefits of distal ventricular pacing in mid-cavity obstructive hypertrophic cardiomyopathy.
Introduction: Hypertrophic cardiomyopathy (HCM) patients with left ventricular (LV) mid-cavity obstruction (LVMCO) often experience severe drug-refractory symptoms thought to be related to intraventricular obstruction. We tested whether ventricular pacing, guided by invasive haemodynamic assessment, reduced LVMCO and improved refractory symptoms.
Methods: Between December 2008 and December 2017, 16 HCM patients with severe refractory symptoms and LVMCO underwent device implantation with haemodynamic pacing study to assess the effect on invasively defined LVMCO gradients. The effect on the gradient of atrioventricular (AV) synchronous pacing from sites including right ventricular (RV) apex and middle cardiac vein (MCV) was retrospectively assessed.
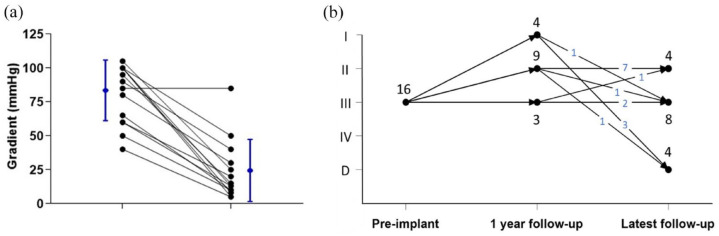
Results: Invasive haemodynamic data were available in 14 of 16 patients. Mean pre-treatment intracavitary gradient was 77 ± 22 mmHg (in sinus rhythm) versus 21 ± 21 mmHg during pacing from optimal ventricular site (95% CI: -70.86 to -40.57, p < 0.0001). Optimal pacing site was distal MCV in 12/16 (86%), RV apex in 1/16 and via epicardial LV lead in 1/16. Pre-pacing Doppler-derived gradients were significantly higher than at follow-up (47 ± 15 versus 24 ± 16 mmHg, 95% CI: -37.19 to -13.73, p < 0.001). Median baseline NYHA class was 3, which had improved by ⩾1 NYHA class in 13 of 16 patients at 1-year post-procedure (p < 0.001). The mean follow-up duration was 4.6 ± 2.7 years with the following outcomes: 8/16 (50%) had continued symptomatic improvement, 4/16 had symptomatic decline and 4/16 died. Contributors to symptomatic decline included chronic atrial fibrillation (AF) (n = 5), phrenic nerve stimulation (n = 3) and ventricular ectopy (n = 1).
Conclusion: In drug-refractory symptomatic LVMCO, distal ventricular pacing can reduce intracavitary obstruction and may provide long-term symptomatic relief in patients with limited treatment options. A haemodynamic pacing study is an effective strategy for identifying optimal pacing site and configuration.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


