Mubin Ozercan, Irem Eser, Saba Kiremitci, Bora Peynircioglu, Selim Karayalcin, Ramazan Idilman
{"title":"免疫球蛋白轻链淀粉样变表现为Budd-Chiari综合征。","authors":"Mubin Ozercan, Irem Eser, Saba Kiremitci, Bora Peynircioglu, Selim Karayalcin, Ramazan Idilman","doi":"10.14744/hf.2021.2021.0028","DOIUrl":null,"url":null,"abstract":"1.7 mg/dL (normal range: 0.3–1 mg/dL), and albumin level of 2.7 g/ dL (normal range: 3.5–5.5 g/dL) were noted. The results of serologi-cal studies for viral hepatitis, an autoimmune panel, and a metabolic panel were all normal. Her D-dimer level was high: 5321 ng/mL (nor-mal range: <250 ng/mL). The antithrombin-III and protein C activity level was 43% (normal range: 70–125%) and 51% (normal range: 70–140%), respectively. Abdominal ultrasonography (US) revealed hepatomegaly and a diffuse increase in parenchyma heterogenicity. Doppler US suggested no flow in the right hepatic vein. Magnetic resonance imaging (MRI) also showed hepatomegaly, a heterogenic liver parenchyma, and no contrast filling in the right hepatic vein, consistent with right hepatic vein occlusion. Anticoagulant therapy with low-molecular-weight heparin was initiated. She was followed-up in the outpatient clinic. She presented at the outpatient clinic in September with fatigue, dyspnea, and abdominal distension. Ascites and peripheral edema were present. Her total bilirubin level had increased to 5.5 mg/dL, immunohistochemistry amyloidosis. proteomics, spectrometry","PeriodicalId":29722,"journal":{"name":"Hepatology Forum","volume":"2 3","pages":"120-121"},"PeriodicalIF":1.2000,"publicationDate":"2021-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/01/hf-2-120.PMC9138943.pdf","citationCount":"0","resultStr":"{\"title\":\"Immunoglobulin light chain amyloidosis presenting as Budd-Chiari syndrome.\",\"authors\":\"Mubin Ozercan, Irem Eser, Saba Kiremitci, Bora Peynircioglu, Selim Karayalcin, Ramazan Idilman\",\"doi\":\"10.14744/hf.2021.2021.0028\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"1.7 mg/dL (normal range: 0.3–1 mg/dL), and albumin level of 2.7 g/ dL (normal range: 3.5–5.5 g/dL) were noted. The results of serologi-cal studies for viral hepatitis, an autoimmune panel, and a metabolic panel were all normal. Her D-dimer level was high: 5321 ng/mL (nor-mal range: <250 ng/mL). The antithrombin-III and protein C activity level was 43% (normal range: 70–125%) and 51% (normal range: 70–140%), respectively. Abdominal ultrasonography (US) revealed hepatomegaly and a diffuse increase in parenchyma heterogenicity. Doppler US suggested no flow in the right hepatic vein. Magnetic resonance imaging (MRI) also showed hepatomegaly, a heterogenic liver parenchyma, and no contrast filling in the right hepatic vein, consistent with right hepatic vein occlusion. Anticoagulant therapy with low-molecular-weight heparin was initiated. She was followed-up in the outpatient clinic. She presented at the outpatient clinic in September with fatigue, dyspnea, and abdominal distension. Ascites and peripheral edema were present. Her total bilirubin level had increased to 5.5 mg/dL, immunohistochemistry amyloidosis. proteomics, spectrometry\",\"PeriodicalId\":29722,\"journal\":{\"name\":\"Hepatology Forum\",\"volume\":\"2 3\",\"pages\":\"120-121\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2021-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/01/hf-2-120.PMC9138943.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hepatology Forum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/hf.2021.2021.0028\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/hf.2021.2021.0028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
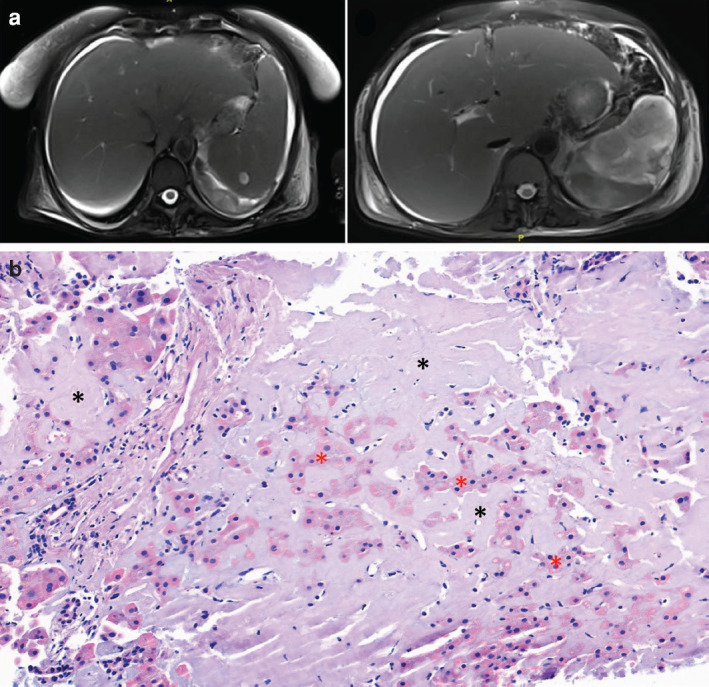
Immunoglobulin light chain amyloidosis presenting as Budd-Chiari syndrome.
1.7 mg/dL (normal range: 0.3–1 mg/dL), and albumin level of 2.7 g/ dL (normal range: 3.5–5.5 g/dL) were noted. The results of serologi-cal studies for viral hepatitis, an autoimmune panel, and a metabolic panel were all normal. Her D-dimer level was high: 5321 ng/mL (nor-mal range: <250 ng/mL). The antithrombin-III and protein C activity level was 43% (normal range: 70–125%) and 51% (normal range: 70–140%), respectively. Abdominal ultrasonography (US) revealed hepatomegaly and a diffuse increase in parenchyma heterogenicity. Doppler US suggested no flow in the right hepatic vein. Magnetic resonance imaging (MRI) also showed hepatomegaly, a heterogenic liver parenchyma, and no contrast filling in the right hepatic vein, consistent with right hepatic vein occlusion. Anticoagulant therapy with low-molecular-weight heparin was initiated. She was followed-up in the outpatient clinic. She presented at the outpatient clinic in September with fatigue, dyspnea, and abdominal distension. Ascites and peripheral edema were present. Her total bilirubin level had increased to 5.5 mg/dL, immunohistochemistry amyloidosis. proteomics, spectrometry

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


