Pranjal Vaidya, Mehdi Alilou, Amogh Hiremath, Amit Gupta, Kaustav Bera, Jennifer Furin, Keith Armitage, Robert Gilkeson, Lei Yuan, Pingfu Fu, Cheng Lu, Mengyao Ji, Anant Madabhushi
{"title":"预测COVID-19患者疾病严重程度和呼吸机支持需求的端到端综合临床和基于ct的放射组学Nomogram:一项大型多地点回顾性研究","authors":"Pranjal Vaidya, Mehdi Alilou, Amogh Hiremath, Amit Gupta, Kaustav Bera, Jennifer Furin, Keith Armitage, Robert Gilkeson, Lei Yuan, Pingfu Fu, Cheng Lu, Mengyao Ji, Anant Madabhushi","doi":"10.3389/fradi.2022.781536","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The disease COVID-19 has caused a widespread global pandemic with ~3. 93 million deaths worldwide. In this work, we present three models-radiomics (M<sub>RM</sub>), clinical (M<sub>CM</sub>), and combined clinical-radiomics (M<sub>RCM</sub>) nomogram to predict COVID-19-positive patients who will end up needing invasive mechanical ventilation from the baseline CT scans.</p><p><strong>Methods: </strong>We performed a retrospective multicohort study of individuals with COVID-19-positive findings for a total of 897 patients from two different institutions (Renmin Hospital of Wuhan University, D<sub>1</sub> = 787, and University Hospitals, US D<sub>2</sub> = 110). The patients from institution-1 were divided into 60% training, <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> <mo>(</mo> <mi>N</mi> <mo>=</mo> <mn>473</mn> <mo>)</mo></mrow> </math> , and 40% test set <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> <mo>(</mo> <mi>N</mi> <mo>=</mo> <mn>314</mn> <mo>)</mo></mrow> </math> . The patients from institution-2 were used for an independent validation test set <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> <mo>(</mo> <mi>N</mi> <mo>=</mo> <mn>110</mn> <mo>)</mo></mrow> </math> . A U-Net-based neural network (CNN) was trained to automatically segment out the COVID consolidation regions on the CT scans. The segmented regions from the CT scans were used for extracting first- and higher-order radiomic textural features. The top radiomic and clinical features were selected using the least absolute shrinkage and selection operator (LASSO) with an optimal binomial regression model within <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> .</p><p><strong>Results: </strong>The three out of the top five features identified using <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> were higher-order textural features (GLCM, GLRLM, GLSZM), whereas the last two features included the total absolute infection size on the CT scan and the total intensity of the COVID consolidations. The radiomics model (M<sub>RM</sub>) was constructed using the radiomic score built using the coefficients obtained from the LASSO logistic model used within the linear regression (LR) classifier. The M<sub>RM</sub> yielded an area under the receiver operating characteristic curve (AUC) of 0.754 (0.709-0.799) on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> , 0.836 on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> , and 0.748 <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> . The top prognostic clinical factors identified in the analysis were dehydrogenase (LDH), age, and albumin (ALB). The clinical model had an AUC of 0.784 (0.743-0.825) on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> , 0.813 on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> , and 0.688 on <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> . Finally, the combined model, M<sub>RCM</sub> integrating radiomic score, age, LDH and ALB, yielded an AUC of 0.814 (0.774-0.853) on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> , 0.847 on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> , and 0.771 on <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> . The M<sub>RCM</sub> had an overall improvement in the performance of ~5.85% ( <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> : <i>p</i> = 0.0031; <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> <i>p</i> = 0.0165; <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> : <i>p</i> = 0.0369) over M<sub>CM</sub>.</p><p><strong>Conclusion: </strong>The novel integrated imaging and clinical model (M<sub>RCM</sub>) outperformed both models (M<sub>RM</sub>) and (M<sub>CM</sub>). Our results across multiple sites suggest that the integrated nomogram could help identify COVID-19 patients with more severe disease phenotype and potentially require mechanical ventilation.</p>","PeriodicalId":73101,"journal":{"name":"Frontiers in radiology","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9696643/pdf/","citationCount":"1","resultStr":"{\"title\":\"An End-to-End Integrated Clinical and CT-Based Radiomics Nomogram for Predicting Disease Severity and Need for Ventilator Support in COVID-19 Patients: A Large Multisite Retrospective Study.\",\"authors\":\"Pranjal Vaidya, Mehdi Alilou, Amogh Hiremath, Amit Gupta, Kaustav Bera, Jennifer Furin, Keith Armitage, Robert Gilkeson, Lei Yuan, Pingfu Fu, Cheng Lu, Mengyao Ji, Anant Madabhushi\",\"doi\":\"10.3389/fradi.2022.781536\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The disease COVID-19 has caused a widespread global pandemic with ~3. 93 million deaths worldwide. In this work, we present three models-radiomics (M<sub>RM</sub>), clinical (M<sub>CM</sub>), and combined clinical-radiomics (M<sub>RCM</sub>) nomogram to predict COVID-19-positive patients who will end up needing invasive mechanical ventilation from the baseline CT scans.</p><p><strong>Methods: </strong>We performed a retrospective multicohort study of individuals with COVID-19-positive findings for a total of 897 patients from two different institutions (Renmin Hospital of Wuhan University, D<sub>1</sub> = 787, and University Hospitals, US D<sub>2</sub> = 110). The patients from institution-1 were divided into 60% training, <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> <mo>(</mo> <mi>N</mi> <mo>=</mo> <mn>473</mn> <mo>)</mo></mrow> </math> , and 40% test set <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> <mo>(</mo> <mi>N</mi> <mo>=</mo> <mn>314</mn> <mo>)</mo></mrow> </math> . The patients from institution-2 were used for an independent validation test set <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> <mo>(</mo> <mi>N</mi> <mo>=</mo> <mn>110</mn> <mo>)</mo></mrow> </math> . A U-Net-based neural network (CNN) was trained to automatically segment out the COVID consolidation regions on the CT scans. The segmented regions from the CT scans were used for extracting first- and higher-order radiomic textural features. The top radiomic and clinical features were selected using the least absolute shrinkage and selection operator (LASSO) with an optimal binomial regression model within <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> .</p><p><strong>Results: </strong>The three out of the top five features identified using <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> were higher-order textural features (GLCM, GLRLM, GLSZM), whereas the last two features included the total absolute infection size on the CT scan and the total intensity of the COVID consolidations. The radiomics model (M<sub>RM</sub>) was constructed using the radiomic score built using the coefficients obtained from the LASSO logistic model used within the linear regression (LR) classifier. The M<sub>RM</sub> yielded an area under the receiver operating characteristic curve (AUC) of 0.754 (0.709-0.799) on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> , 0.836 on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> , and 0.748 <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> . The top prognostic clinical factors identified in the analysis were dehydrogenase (LDH), age, and albumin (ALB). The clinical model had an AUC of 0.784 (0.743-0.825) on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> , 0.813 on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> , and 0.688 on <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> . Finally, the combined model, M<sub>RCM</sub> integrating radiomic score, age, LDH and ALB, yielded an AUC of 0.814 (0.774-0.853) on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> , 0.847 on <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> , and 0.771 on <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> . The M<sub>RCM</sub> had an overall improvement in the performance of ~5.85% ( <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>T</mtext></msubsup> </mrow> </math> : <i>p</i> = 0.0031; <math> <mrow><msubsup><mtext>D</mtext> <mn>1</mn> <mtext>V</mtext></msubsup> </mrow> </math> <i>p</i> = 0.0165; <math> <mrow><msubsup><mtext>D</mtext> <mn>2</mn> <mtext>V</mtext></msubsup> </mrow> </math> : <i>p</i> = 0.0369) over M<sub>CM</sub>.</p><p><strong>Conclusion: </strong>The novel integrated imaging and clinical model (M<sub>RCM</sub>) outperformed both models (M<sub>RM</sub>) and (M<sub>CM</sub>). Our results across multiple sites suggest that the integrated nomogram could help identify COVID-19 patients with more severe disease phenotype and potentially require mechanical ventilation.</p>\",\"PeriodicalId\":73101,\"journal\":{\"name\":\"Frontiers in radiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9696643/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fradi.2022.781536\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/4/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fradi.2022.781536","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/4/8 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
目的:新型冠状病毒病(COVID-19)已在全球范围内引起大流行。全世界9300万人死亡。在这项工作中,我们提出了三种模型-放射组学(MRM),临床(MCM)和临床-放射组学(MRCM)联合nomogram来预测covid -19阳性患者,这些患者最终需要从基线CT扫描中获得有创机械通气。方法:对来自武汉大学人民医院(D1 = 787)和美国大学附属医院(D2 = 110)的897例covid -19阳性个体进行回顾性多队列研究。1机构患者分为60%训练组、d1组(N = 473)和40%测试组d1组(N = 314)。来自第二机构的患者被用于独立验证试验集d2 V (N = 110)。训练基于u - net的神经网络(CNN),自动分割出CT扫描上的COVID巩固区域。CT扫描的分割区域用于提取一阶和高阶放射学纹理特征。使用最小绝对收缩和选择算子(LASSO)和最佳二项回归模型在d1 T内选择放射学和临床特征。结果:使用d1 T确定的前五个特征中有三个是高阶纹理特征(GLCM, GLRLM, GLSZM),而最后两个特征包括CT扫描上的总绝对感染大小和COVID巩固的总强度。利用线性回归(LR)分类器中使用的LASSO逻辑模型获得的系数构建放射组学评分,构建放射组学模型(MRM)。MRM在d1 T、d1 V和d2 V下的AUC分别为0.754(0.709-0.799)、0.836和0.748。在分析中确定的最重要的预后临床因素是脱氢酶(LDH)、年龄和白蛋白(ALB)。临床模型d1 T、d1 V、d2 V的AUC分别为0.784(0.743 ~ 0.825)、0.813和0.688。最后,综合放射学评分、年龄、LDH和ALB的MRCM组合模型在d1上的AUC为0.814 (0.774-0.853),d1上的AUC为0.847,d2上的AUC为0.771。MRCM的整体性能改善约5.85% (d1: p = 0.0031;d1 V p = 0.0165;d2v: p = 0.0369)大于MCM。结论:新型影像与临床综合模型(MRCM)优于MRM和MCM两种模型。我们在多个地点的研究结果表明,综合nomograph可以帮助识别疾病表型更严重且可能需要机械通气的COVID-19患者。
An End-to-End Integrated Clinical and CT-Based Radiomics Nomogram for Predicting Disease Severity and Need for Ventilator Support in COVID-19 Patients: A Large Multisite Retrospective Study.
Objective: The disease COVID-19 has caused a widespread global pandemic with ~3. 93 million deaths worldwide. In this work, we present three models-radiomics (MRM), clinical (MCM), and combined clinical-radiomics (MRCM) nomogram to predict COVID-19-positive patients who will end up needing invasive mechanical ventilation from the baseline CT scans.
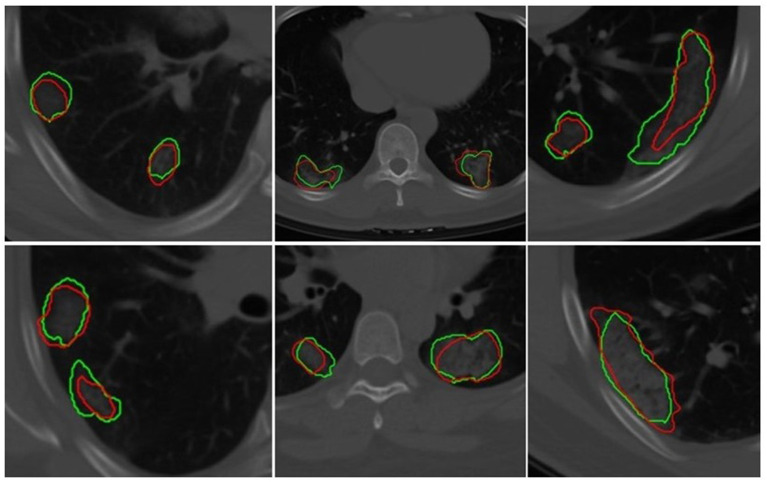
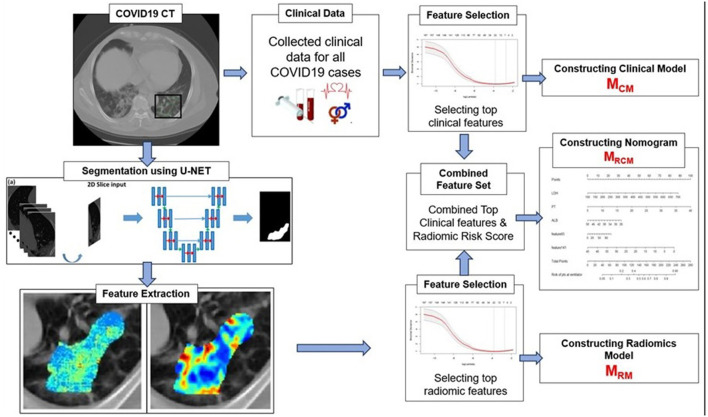
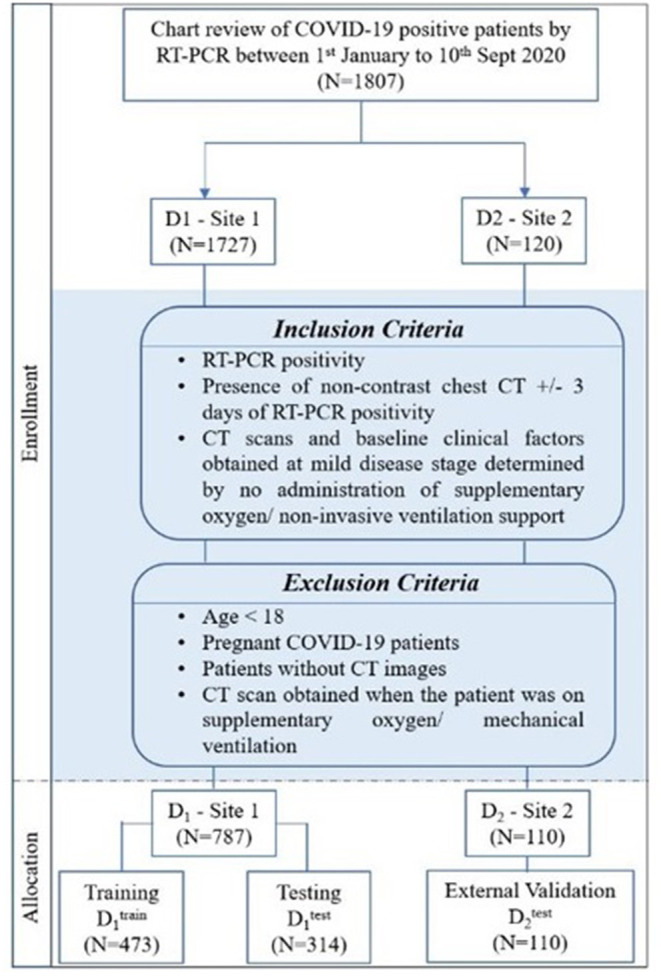
Methods: We performed a retrospective multicohort study of individuals with COVID-19-positive findings for a total of 897 patients from two different institutions (Renmin Hospital of Wuhan University, D1 = 787, and University Hospitals, US D2 = 110). The patients from institution-1 were divided into 60% training, , and 40% test set . The patients from institution-2 were used for an independent validation test set . A U-Net-based neural network (CNN) was trained to automatically segment out the COVID consolidation regions on the CT scans. The segmented regions from the CT scans were used for extracting first- and higher-order radiomic textural features. The top radiomic and clinical features were selected using the least absolute shrinkage and selection operator (LASSO) with an optimal binomial regression model within .
Results: The three out of the top five features identified using were higher-order textural features (GLCM, GLRLM, GLSZM), whereas the last two features included the total absolute infection size on the CT scan and the total intensity of the COVID consolidations. The radiomics model (MRM) was constructed using the radiomic score built using the coefficients obtained from the LASSO logistic model used within the linear regression (LR) classifier. The MRM yielded an area under the receiver operating characteristic curve (AUC) of 0.754 (0.709-0.799) on , 0.836 on , and 0.748 . The top prognostic clinical factors identified in the analysis were dehydrogenase (LDH), age, and albumin (ALB). The clinical model had an AUC of 0.784 (0.743-0.825) on , 0.813 on , and 0.688 on . Finally, the combined model, MRCM integrating radiomic score, age, LDH and ALB, yielded an AUC of 0.814 (0.774-0.853) on , 0.847 on , and 0.771 on . The MRCM had an overall improvement in the performance of ~5.85% ( : p = 0.0031; p = 0.0165; : p = 0.0369) over MCM.
Conclusion: The novel integrated imaging and clinical model (MRCM) outperformed both models (MRM) and (MCM). Our results across multiple sites suggest that the integrated nomogram could help identify COVID-19 patients with more severe disease phenotype and potentially require mechanical ventilation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


