{"title":"Graves病治疗后立即并发不典型心绞痛和长QT综合征的心室颤动1例","authors":"Hajime Iwasaki, Hirotsugu Suwanai, Hiroyuki Sakai, Keitaro Ishii, Natsuko Hara, Kazuhiro Satomi, Yasuyuki Takada, Yuki Nagamatsu, Ryo Suzuki","doi":"10.1186/s13044-022-00136-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Palpitations due to Graves' disease are often caused by supraventricular arrhythmia. However, in rare cases, the background of coronary artery disease, genetic abnormalities, or channel abnormalities can cause ventricular fibrillation, which is a lethal arrhythmia. Here, we report a case of ventricular fibrillation after administration of beta-blockers early in the course of treatment for Graves' disease coexisting with atypical angina and long QT syndrome.</p><p><strong>Case presentation: </strong>A 48-year-old man consulted a local general physician for chest discomfort and palpitations for approximately 2 weeks. He was diagnosed with Graves' disease and treated with thiamazole 15 mg, bisoprolol 1.25 mg, and nitroglycerin 0.3 mg. The patient continued to experience chest discomfort the next day and visited our hospital. The patient was treated with landiolol 0.125 mg/kg/min for heart rate control, and 20 min later, electrocardiography showed a change from the R-on-T phenomenon to ventricular fibrillation. After cardiopulmonary resumption and improvement of thyroid function, a stress test was performed, which revealed coronary angina and long QT syndrome. An implantable cardioverter defibrillator (ICD) was implanted in the patient for secondary prevention. Since then, no fatal arrhythmia has been observed to date.</p><p><strong>Conclusions: </strong>When beta-blockers are administered to patients with Graves' disease who have severe chest symptoms, fatal arrhythmias are possible. ICD implantation should be considered for the secondary prevention of fatal arrhythmias.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":null,"pages":null},"PeriodicalIF":1.9000,"publicationDate":"2022-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9528117/pdf/","citationCount":"1","resultStr":"{\"title\":\"Ventricular fibrillation immediately after the treatment of Graves' disease coexisting with atypical angina and long QT syndrome: a case report.\",\"authors\":\"Hajime Iwasaki, Hirotsugu Suwanai, Hiroyuki Sakai, Keitaro Ishii, Natsuko Hara, Kazuhiro Satomi, Yasuyuki Takada, Yuki Nagamatsu, Ryo Suzuki\",\"doi\":\"10.1186/s13044-022-00136-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Palpitations due to Graves' disease are often caused by supraventricular arrhythmia. However, in rare cases, the background of coronary artery disease, genetic abnormalities, or channel abnormalities can cause ventricular fibrillation, which is a lethal arrhythmia. Here, we report a case of ventricular fibrillation after administration of beta-blockers early in the course of treatment for Graves' disease coexisting with atypical angina and long QT syndrome.</p><p><strong>Case presentation: </strong>A 48-year-old man consulted a local general physician for chest discomfort and palpitations for approximately 2 weeks. He was diagnosed with Graves' disease and treated with thiamazole 15 mg, bisoprolol 1.25 mg, and nitroglycerin 0.3 mg. The patient continued to experience chest discomfort the next day and visited our hospital. The patient was treated with landiolol 0.125 mg/kg/min for heart rate control, and 20 min later, electrocardiography showed a change from the R-on-T phenomenon to ventricular fibrillation. After cardiopulmonary resumption and improvement of thyroid function, a stress test was performed, which revealed coronary angina and long QT syndrome. An implantable cardioverter defibrillator (ICD) was implanted in the patient for secondary prevention. Since then, no fatal arrhythmia has been observed to date.</p><p><strong>Conclusions: </strong>When beta-blockers are administered to patients with Graves' disease who have severe chest symptoms, fatal arrhythmias are possible. ICD implantation should be considered for the secondary prevention of fatal arrhythmias.</p>\",\"PeriodicalId\":39048,\"journal\":{\"name\":\"Thyroid Research\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2022-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9528117/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thyroid Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13044-022-00136-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-022-00136-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Ventricular fibrillation immediately after the treatment of Graves' disease coexisting with atypical angina and long QT syndrome: a case report.
Background: Palpitations due to Graves' disease are often caused by supraventricular arrhythmia. However, in rare cases, the background of coronary artery disease, genetic abnormalities, or channel abnormalities can cause ventricular fibrillation, which is a lethal arrhythmia. Here, we report a case of ventricular fibrillation after administration of beta-blockers early in the course of treatment for Graves' disease coexisting with atypical angina and long QT syndrome.
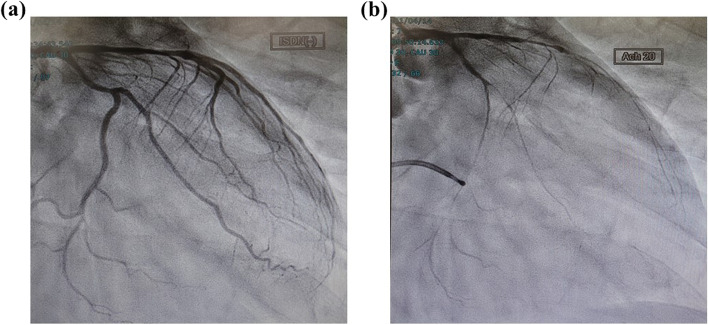
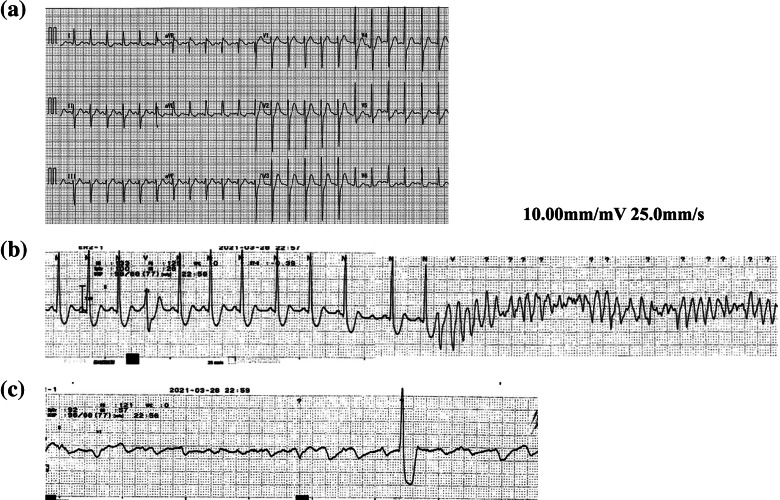
Case presentation: A 48-year-old man consulted a local general physician for chest discomfort and palpitations for approximately 2 weeks. He was diagnosed with Graves' disease and treated with thiamazole 15 mg, bisoprolol 1.25 mg, and nitroglycerin 0.3 mg. The patient continued to experience chest discomfort the next day and visited our hospital. The patient was treated with landiolol 0.125 mg/kg/min for heart rate control, and 20 min later, electrocardiography showed a change from the R-on-T phenomenon to ventricular fibrillation. After cardiopulmonary resumption and improvement of thyroid function, a stress test was performed, which revealed coronary angina and long QT syndrome. An implantable cardioverter defibrillator (ICD) was implanted in the patient for secondary prevention. Since then, no fatal arrhythmia has been observed to date.
Conclusions: When beta-blockers are administered to patients with Graves' disease who have severe chest symptoms, fatal arrhythmias are possible. ICD implantation should be considered for the secondary prevention of fatal arrhythmias.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


