Isabella Sjölander , Anna Borgström , Pia Nerfeldt , Danielle Friberg
{"title":"儿童阻塞性睡眠呼吸暂停的腺扁桃体切除术与腺扁桃体切除术:一项5年的随机对照试验","authors":"Isabella Sjölander , Anna Borgström , Pia Nerfeldt , Danielle Friberg","doi":"10.1016/j.sleepx.2022.100055","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><p>Adenotonsillectomy (ATE) is a common treatment for pediatric obstructive sleep apnea (OSA). Intracapsular adenotonsillotomy (ATT) is associated with less postoperative morbidity. Our previous randomized controlled trial (RCT) compared ATE and ATT in otherwise healthy children with moderate to severe OSA. No differences in polysomnographic (PSG) and OSA-18 were found between the groups at one-year follow-up. This study presents the long-term results of the RCT.</p></div><div><h3>Methods</h3><p>Non-obese children (n = 79, 2–6 years) who had undergone either ATE (n = 40) or ATT (n = 39) were offered PSG and OSA-18 questionnaire five-years after surgery. Primary outcome was the group difference in postoperative Obstructive Apnea/Hypopnea Index (OAHI). ATE was recommended to the ATT group if they had a relapse of OSA.</p></div><div><h3>Results</h3><p>The follow-up was completed by 45 of 79 (57%) children; 28 (35%) drop-outs, and six of 39(15%) in the ATT group were excluded after ATE. After ATE(n = 17), OAHI decreased from mean 12.3(SD 8.0) to 0.6(0.7), and after ATT(n = 28) from 12.6(7.4) to 0.5(0.6), a mean difference in postoperative OAHI of 0.1(95% CI -0.3 – 0.5). Sensitivity analyses did not change the results. The median OSA-18 decreased in the ATE group from 57(interquartile range 47–79) to 27(22–36), and in the ATT group from 67(53–79) to 32(25–44), without group differences for postoperative values.</p></div><div><h3>Conclusion</h3><p>The results of this five-year follow-up of otherwise healthy OSA-children showed a high drop-out rate, but indicates that ATT could be an effective treatment for pediatric OSA. However, ATT warrants follow-up due to the risk of recurrence, and further studies are needed.</p></div>","PeriodicalId":37065,"journal":{"name":"Sleep Medicine: X","volume":"4 ","pages":"Article 100055"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9482134/pdf/","citationCount":"1","resultStr":"{\"title\":\"Adenotonsillotomy versus adenotonsillectomy in pediatric obstructive sleep apnea: A 5-year RCT\",\"authors\":\"Isabella Sjölander , Anna Borgström , Pia Nerfeldt , Danielle Friberg\",\"doi\":\"10.1016/j.sleepx.2022.100055\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><p>Adenotonsillectomy (ATE) is a common treatment for pediatric obstructive sleep apnea (OSA). Intracapsular adenotonsillotomy (ATT) is associated with less postoperative morbidity. Our previous randomized controlled trial (RCT) compared ATE and ATT in otherwise healthy children with moderate to severe OSA. No differences in polysomnographic (PSG) and OSA-18 were found between the groups at one-year follow-up. This study presents the long-term results of the RCT.</p></div><div><h3>Methods</h3><p>Non-obese children (n = 79, 2–6 years) who had undergone either ATE (n = 40) or ATT (n = 39) were offered PSG and OSA-18 questionnaire five-years after surgery. Primary outcome was the group difference in postoperative Obstructive Apnea/Hypopnea Index (OAHI). ATE was recommended to the ATT group if they had a relapse of OSA.</p></div><div><h3>Results</h3><p>The follow-up was completed by 45 of 79 (57%) children; 28 (35%) drop-outs, and six of 39(15%) in the ATT group were excluded after ATE. After ATE(n = 17), OAHI decreased from mean 12.3(SD 8.0) to 0.6(0.7), and after ATT(n = 28) from 12.6(7.4) to 0.5(0.6), a mean difference in postoperative OAHI of 0.1(95% CI -0.3 – 0.5). Sensitivity analyses did not change the results. The median OSA-18 decreased in the ATE group from 57(interquartile range 47–79) to 27(22–36), and in the ATT group from 67(53–79) to 32(25–44), without group differences for postoperative values.</p></div><div><h3>Conclusion</h3><p>The results of this five-year follow-up of otherwise healthy OSA-children showed a high drop-out rate, but indicates that ATT could be an effective treatment for pediatric OSA. However, ATT warrants follow-up due to the risk of recurrence, and further studies are needed.</p></div>\",\"PeriodicalId\":37065,\"journal\":{\"name\":\"Sleep Medicine: X\",\"volume\":\"4 \",\"pages\":\"Article 100055\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9482134/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Sleep Medicine: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590142722000143\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sleep Medicine: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590142722000143","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Adenotonsillotomy versus adenotonsillectomy in pediatric obstructive sleep apnea: A 5-year RCT
Objectives
Adenotonsillectomy (ATE) is a common treatment for pediatric obstructive sleep apnea (OSA). Intracapsular adenotonsillotomy (ATT) is associated with less postoperative morbidity. Our previous randomized controlled trial (RCT) compared ATE and ATT in otherwise healthy children with moderate to severe OSA. No differences in polysomnographic (PSG) and OSA-18 were found between the groups at one-year follow-up. This study presents the long-term results of the RCT.
Methods
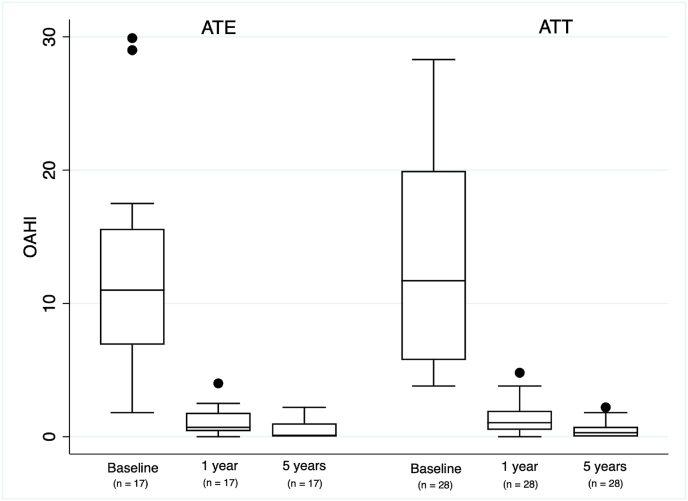
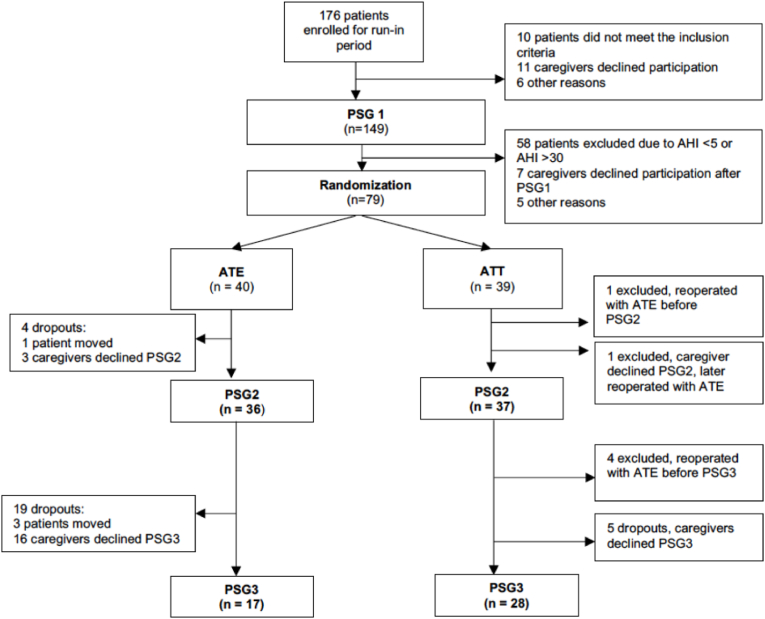
Non-obese children (n = 79, 2–6 years) who had undergone either ATE (n = 40) or ATT (n = 39) were offered PSG and OSA-18 questionnaire five-years after surgery. Primary outcome was the group difference in postoperative Obstructive Apnea/Hypopnea Index (OAHI). ATE was recommended to the ATT group if they had a relapse of OSA.
Results
The follow-up was completed by 45 of 79 (57%) children; 28 (35%) drop-outs, and six of 39(15%) in the ATT group were excluded after ATE. After ATE(n = 17), OAHI decreased from mean 12.3(SD 8.0) to 0.6(0.7), and after ATT(n = 28) from 12.6(7.4) to 0.5(0.6), a mean difference in postoperative OAHI of 0.1(95% CI -0.3 – 0.5). Sensitivity analyses did not change the results. The median OSA-18 decreased in the ATE group from 57(interquartile range 47–79) to 27(22–36), and in the ATT group from 67(53–79) to 32(25–44), without group differences for postoperative values.
Conclusion
The results of this five-year follow-up of otherwise healthy OSA-children showed a high drop-out rate, but indicates that ATT could be an effective treatment for pediatric OSA. However, ATT warrants follow-up due to the risk of recurrence, and further studies are needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


