Sukaina Hasnie, Chad Glenn, Jo E G Peterson, Edward T El Rassi, Kibwei A McKinney
{"title":"高级别双表型鼻窦肉瘤1例报告。","authors":"Sukaina Hasnie, Chad Glenn, Jo E G Peterson, Edward T El Rassi, Kibwei A McKinney","doi":"10.1055/s-0042-1755599","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> Biphenotypic sinonasal sarcoma (BSNS) is a recently found entity that first described by Lewis et al. It was then added to the 4th edition of the World Health Organization (WHO) of head and neck tumors in 2012. BSNS has been described as a rare low-grade sarcoma arising in the upper sinonasal tract. It is believed that in the past, BSNS was, likely, previously diagnosed as other low-grade or benign malignancies. Fibrosarcoma, leiomyosarcoma, and peripheral nerve sheath tumors, all fall within the differential diagnosis of BSNS. However, BSNS is unlike other mesenchymal sinonasal tumors, as it displays both neural and myogenic differentiation. BSNS has thus far been recognized in only a hand full of case reports, all of which have reported similar morphologic features of a low-grade soft tissue tumor with neural involvement arising from the nasal cavity or ethmoid air cells in middle aged individuals. In fact, being low-grade sarcoma became such a hallmark characteristic of this tumor that it even received the name low-grade sinonasal sarcoma with neural and myogenic features or LGSSNMF. <b>Case Presentation</b> We present, however, for the first time, a high-grade differentiation of BSNS in an otherwise healthy 72-year-old female. The patient was referred from an outside ENT (ear, nose, and throat) after pathology from a presumed polypectomy returned positive for a BSNS. Initial imaging revealed erosion through the bilateral lamina papyracea, anterior cranial fossa floor, and posterior table of the frontal sinus. She then underwent a combined endoscopic and bicoronal open approach for resection of the skull base lesion that was found to encompass the entirety of the sinonasal cavities bilaterally. Postoperatively, the patient underwent significant complications including infection of the pericranial flap, pneumocephalus, and eventually death. <b>Discussion</b> As BSNS is a fairly new entity, currently there has only been four case series conducted, each identifying features of a low-grade sarcoma with both myogenic and neural differentiation. Histologically, BSNS has monophasic spindle cells with uniform, elongated nuclei with scant cytoplasm between benign proliferations of surface-type respiratory epithelium, with a low mitotic rate. Our case, however, revealed pleomorphic hyperchromatic cells with high mitotic activity and necrosis with invasion of bone, staging it as high grade. Immunohistochemistry also differed from the previously reported standards. This case describes a new category for BSNS which may change the differential diagnosis, management, and surgical recommendations that are currently utilized for this skull base neoplasm.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":" ","pages":"e105-e109"},"PeriodicalIF":0.7000,"publicationDate":"2022-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9d/8c/10-1055-s-0042-1755599.PMC9470382.pdf","citationCount":"4","resultStr":"{\"title\":\"High-Grade Biphenotypic Sinonasal Sarcoma: A Case Report.\",\"authors\":\"Sukaina Hasnie, Chad Glenn, Jo E G Peterson, Edward T El Rassi, Kibwei A McKinney\",\"doi\":\"10.1055/s-0042-1755599\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b> Biphenotypic sinonasal sarcoma (BSNS) is a recently found entity that first described by Lewis et al. It was then added to the 4th edition of the World Health Organization (WHO) of head and neck tumors in 2012. BSNS has been described as a rare low-grade sarcoma arising in the upper sinonasal tract. It is believed that in the past, BSNS was, likely, previously diagnosed as other low-grade or benign malignancies. Fibrosarcoma, leiomyosarcoma, and peripheral nerve sheath tumors, all fall within the differential diagnosis of BSNS. However, BSNS is unlike other mesenchymal sinonasal tumors, as it displays both neural and myogenic differentiation. BSNS has thus far been recognized in only a hand full of case reports, all of which have reported similar morphologic features of a low-grade soft tissue tumor with neural involvement arising from the nasal cavity or ethmoid air cells in middle aged individuals. In fact, being low-grade sarcoma became such a hallmark characteristic of this tumor that it even received the name low-grade sinonasal sarcoma with neural and myogenic features or LGSSNMF. <b>Case Presentation</b> We present, however, for the first time, a high-grade differentiation of BSNS in an otherwise healthy 72-year-old female. The patient was referred from an outside ENT (ear, nose, and throat) after pathology from a presumed polypectomy returned positive for a BSNS. Initial imaging revealed erosion through the bilateral lamina papyracea, anterior cranial fossa floor, and posterior table of the frontal sinus. She then underwent a combined endoscopic and bicoronal open approach for resection of the skull base lesion that was found to encompass the entirety of the sinonasal cavities bilaterally. Postoperatively, the patient underwent significant complications including infection of the pericranial flap, pneumocephalus, and eventually death. <b>Discussion</b> As BSNS is a fairly new entity, currently there has only been four case series conducted, each identifying features of a low-grade sarcoma with both myogenic and neural differentiation. Histologically, BSNS has monophasic spindle cells with uniform, elongated nuclei with scant cytoplasm between benign proliferations of surface-type respiratory epithelium, with a low mitotic rate. Our case, however, revealed pleomorphic hyperchromatic cells with high mitotic activity and necrosis with invasion of bone, staging it as high grade. Immunohistochemistry also differed from the previously reported standards. This case describes a new category for BSNS which may change the differential diagnosis, management, and surgical recommendations that are currently utilized for this skull base neoplasm.</p>\",\"PeriodicalId\":44256,\"journal\":{\"name\":\"Journal of Neurological Surgery Reports\",\"volume\":\" \",\"pages\":\"e105-e109\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9d/8c/10-1055-s-0042-1755599.PMC9470382.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurological Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0042-1755599\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1755599","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
High-Grade Biphenotypic Sinonasal Sarcoma: A Case Report.
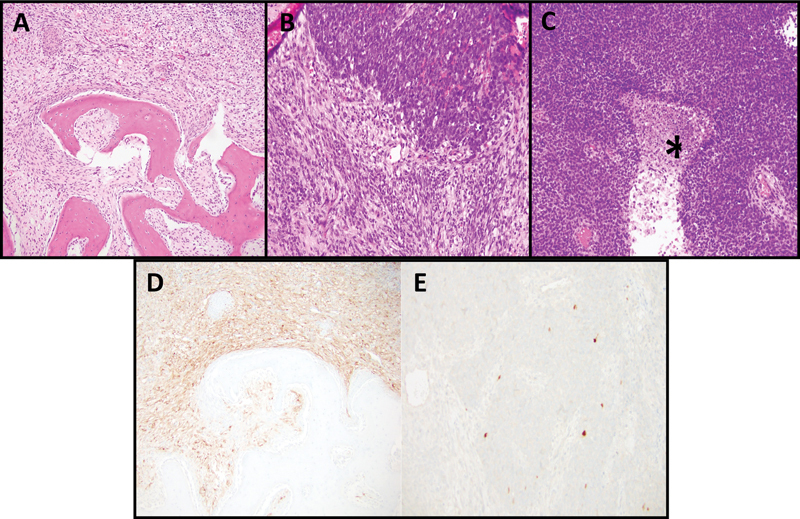
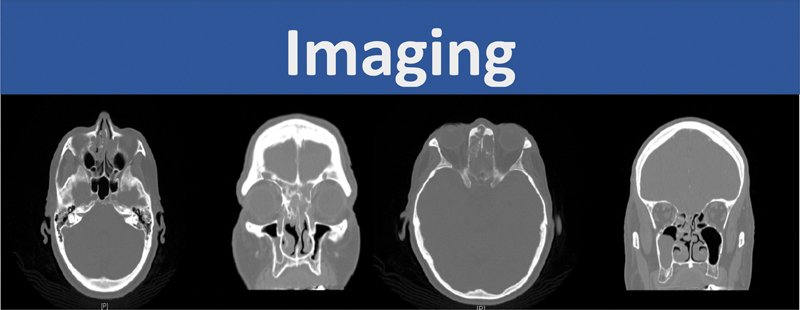
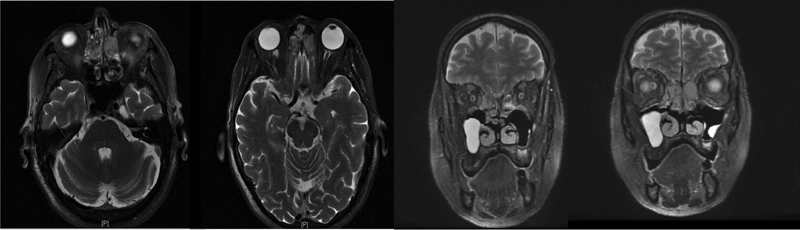
Introduction Biphenotypic sinonasal sarcoma (BSNS) is a recently found entity that first described by Lewis et al. It was then added to the 4th edition of the World Health Organization (WHO) of head and neck tumors in 2012. BSNS has been described as a rare low-grade sarcoma arising in the upper sinonasal tract. It is believed that in the past, BSNS was, likely, previously diagnosed as other low-grade or benign malignancies. Fibrosarcoma, leiomyosarcoma, and peripheral nerve sheath tumors, all fall within the differential diagnosis of BSNS. However, BSNS is unlike other mesenchymal sinonasal tumors, as it displays both neural and myogenic differentiation. BSNS has thus far been recognized in only a hand full of case reports, all of which have reported similar morphologic features of a low-grade soft tissue tumor with neural involvement arising from the nasal cavity or ethmoid air cells in middle aged individuals. In fact, being low-grade sarcoma became such a hallmark characteristic of this tumor that it even received the name low-grade sinonasal sarcoma with neural and myogenic features or LGSSNMF. Case Presentation We present, however, for the first time, a high-grade differentiation of BSNS in an otherwise healthy 72-year-old female. The patient was referred from an outside ENT (ear, nose, and throat) after pathology from a presumed polypectomy returned positive for a BSNS. Initial imaging revealed erosion through the bilateral lamina papyracea, anterior cranial fossa floor, and posterior table of the frontal sinus. She then underwent a combined endoscopic and bicoronal open approach for resection of the skull base lesion that was found to encompass the entirety of the sinonasal cavities bilaterally. Postoperatively, the patient underwent significant complications including infection of the pericranial flap, pneumocephalus, and eventually death. Discussion As BSNS is a fairly new entity, currently there has only been four case series conducted, each identifying features of a low-grade sarcoma with both myogenic and neural differentiation. Histologically, BSNS has monophasic spindle cells with uniform, elongated nuclei with scant cytoplasm between benign proliferations of surface-type respiratory epithelium, with a low mitotic rate. Our case, however, revealed pleomorphic hyperchromatic cells with high mitotic activity and necrosis with invasion of bone, staging it as high grade. Immunohistochemistry also differed from the previously reported standards. This case describes a new category for BSNS which may change the differential diagnosis, management, and surgical recommendations that are currently utilized for this skull base neoplasm.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


