Jelle D M Bouwens, Erik W M A Bischoff, Johannes C C M In 't Veen, Tjard R Schermer
{"title":"在初级保健中使用肺功能测试诊断哮喘和COPD的区别。","authors":"Jelle D M Bouwens, Erik W M A Bischoff, Johannes C C M In 't Veen, Tjard R Schermer","doi":"10.1038/s41533-022-00298-4","DOIUrl":null,"url":null,"abstract":"<p><p>Asthma and COPD are defined as different disease entities, but in practice patients often show features of both diseases making it challenging for primary care clinicians to establish a correct diagnosis. We aimed to establish the added value of spirometry and more advanced lung function measurements to differentiate between asthma and COPD. A cross-sectional study in 10 Dutch general practices was performed. 532 subjects were extensively screened on respiratory symptoms and lung function. Two chest physicians assessed if asthma or COPD was present. Using multivariable logistic regression analysis we assessed the ability of three scenarios (i.e. only patient history; diagnostics available to primary care; diagnostics available only to secondary care) to differentiate between the two conditions. Receiver operator characteristics (ROC) curves and area under the curve (AUC) were calculated for each scenario, with the chest physicians' assessment as golden standard. Results showed that 84 subjects were diagnosed with asthma, 138 with COPD, and 310 with no chronic respiratory disease. In the scenario including only patient history items, ROC characteristics of the model showed an AUC of 0.84 (95% CI 0.78-0.89) for differentiation between asthma and COPD. When adding diagnostics available to primary care (i.e., pre- and postbronchodilator spirometry) AUC increased to 0.89 (95% CI 0.84-0.93; p = 0.020). When adding more advanced secondary care diagnostic tests AUC remained 0.89 (95% CI 0.85-0.94; p = 0.967). We conclude that primary care clinicians' ability to differentiate between asthma and COPD is enhanced by spirometry testing. More advanced diagnostic tests used in hospital care settings do not seem to provide a better overall diagnostic differentiation between asthma and COPD in primary care patients.</p>","PeriodicalId":19470,"journal":{"name":"NPJ Primary Care Respiratory Medicine","volume":null,"pages":null},"PeriodicalIF":3.1000,"publicationDate":"2022-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9445018/pdf/","citationCount":"5","resultStr":"{\"title\":\"Diagnostic differentiation between asthma and COPD in primary care using lung function testing.\",\"authors\":\"Jelle D M Bouwens, Erik W M A Bischoff, Johannes C C M In 't Veen, Tjard R Schermer\",\"doi\":\"10.1038/s41533-022-00298-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Asthma and COPD are defined as different disease entities, but in practice patients often show features of both diseases making it challenging for primary care clinicians to establish a correct diagnosis. We aimed to establish the added value of spirometry and more advanced lung function measurements to differentiate between asthma and COPD. A cross-sectional study in 10 Dutch general practices was performed. 532 subjects were extensively screened on respiratory symptoms and lung function. Two chest physicians assessed if asthma or COPD was present. Using multivariable logistic regression analysis we assessed the ability of three scenarios (i.e. only patient history; diagnostics available to primary care; diagnostics available only to secondary care) to differentiate between the two conditions. Receiver operator characteristics (ROC) curves and area under the curve (AUC) were calculated for each scenario, with the chest physicians' assessment as golden standard. Results showed that 84 subjects were diagnosed with asthma, 138 with COPD, and 310 with no chronic respiratory disease. In the scenario including only patient history items, ROC characteristics of the model showed an AUC of 0.84 (95% CI 0.78-0.89) for differentiation between asthma and COPD. When adding diagnostics available to primary care (i.e., pre- and postbronchodilator spirometry) AUC increased to 0.89 (95% CI 0.84-0.93; p = 0.020). When adding more advanced secondary care diagnostic tests AUC remained 0.89 (95% CI 0.85-0.94; p = 0.967). We conclude that primary care clinicians' ability to differentiate between asthma and COPD is enhanced by spirometry testing. More advanced diagnostic tests used in hospital care settings do not seem to provide a better overall diagnostic differentiation between asthma and COPD in primary care patients.</p>\",\"PeriodicalId\":19470,\"journal\":{\"name\":\"NPJ Primary Care Respiratory Medicine\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2022-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9445018/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Primary Care Respiratory Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41533-022-00298-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Primary Care Respiratory Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41533-022-00298-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 5
摘要
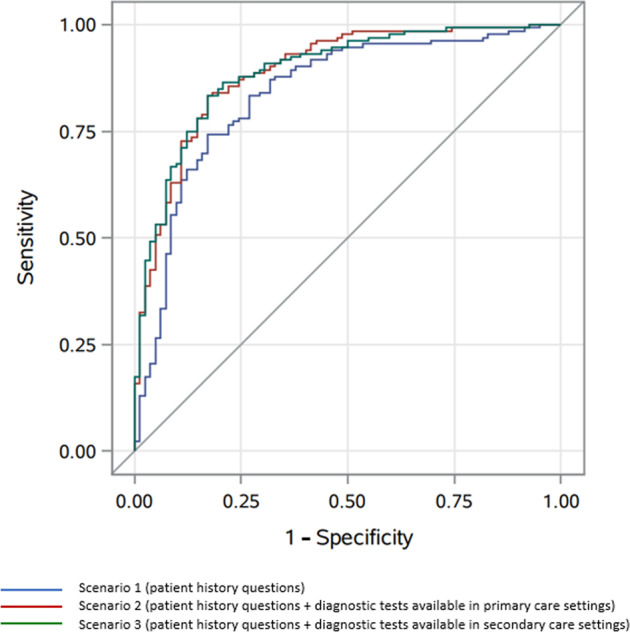
哮喘和慢性阻塞性肺病被定义为不同的疾病实体,但在实践中,患者往往表现出两种疾病的特征,这使得初级保健临床医生很难做出正确的诊断。我们的目的是建立肺量测定和更先进的肺功能测量的附加价值,以区分哮喘和COPD。对10个荷兰全科诊所进行了横断面研究。对532名受试者进行呼吸道症状和肺功能的广泛筛查。两名胸科医生评估患者是否存在哮喘或慢性阻塞性肺病。使用多变量逻辑回归分析,我们评估了三种情况的能力(即只有患者病史;初级保健可获得的诊断;诊断只提供给二级保健),以区分两种情况。以胸科医生的评估为金标准,计算每种情况的受试者操作者特征(ROC)曲线和曲线下面积(AUC)。结果显示,84名受试者被诊断为哮喘,138名受试者被诊断为慢性阻塞性肺病,310名受试者无慢性呼吸道疾病。在仅包括患者病史项目的情况下,模型的ROC特征显示哮喘和COPD区分的AUC为0.84 (95% CI 0.78-0.89)。当增加初级保健可用的诊断(即支气管扩张剂前和后肺活量测定)时,AUC增加到0.89 (95% CI 0.84-0.93;p = 0.020)。当增加更高级的二级保健诊断试验时,AUC仍为0.89 (95% CI 0.85-0.94;p = 0.967)。我们的结论是,初级保健临床医生区分哮喘和COPD的能力可以通过肺活量测定法增强。在医院护理环境中使用的更先进的诊断测试似乎不能更好地对初级保健患者的哮喘和慢性阻塞性肺病进行全面的诊断区分。
Diagnostic differentiation between asthma and COPD in primary care using lung function testing.
Asthma and COPD are defined as different disease entities, but in practice patients often show features of both diseases making it challenging for primary care clinicians to establish a correct diagnosis. We aimed to establish the added value of spirometry and more advanced lung function measurements to differentiate between asthma and COPD. A cross-sectional study in 10 Dutch general practices was performed. 532 subjects were extensively screened on respiratory symptoms and lung function. Two chest physicians assessed if asthma or COPD was present. Using multivariable logistic regression analysis we assessed the ability of three scenarios (i.e. only patient history; diagnostics available to primary care; diagnostics available only to secondary care) to differentiate between the two conditions. Receiver operator characteristics (ROC) curves and area under the curve (AUC) were calculated for each scenario, with the chest physicians' assessment as golden standard. Results showed that 84 subjects were diagnosed with asthma, 138 with COPD, and 310 with no chronic respiratory disease. In the scenario including only patient history items, ROC characteristics of the model showed an AUC of 0.84 (95% CI 0.78-0.89) for differentiation between asthma and COPD. When adding diagnostics available to primary care (i.e., pre- and postbronchodilator spirometry) AUC increased to 0.89 (95% CI 0.84-0.93; p = 0.020). When adding more advanced secondary care diagnostic tests AUC remained 0.89 (95% CI 0.85-0.94; p = 0.967). We conclude that primary care clinicians' ability to differentiate between asthma and COPD is enhanced by spirometry testing. More advanced diagnostic tests used in hospital care settings do not seem to provide a better overall diagnostic differentiation between asthma and COPD in primary care patients.
期刊介绍:
npj Primary Care Respiratory Medicine is an open access, online-only, multidisciplinary journal dedicated to publishing high-quality research in all areas of the primary care management of respiratory and respiratory-related allergic diseases. Papers published by the journal represent important advances of significance to specialists within the fields of primary care and respiratory medicine. We are particularly interested in receiving papers in relation to the following aspects of respiratory medicine, respiratory-related allergic diseases and tobacco control:
epidemiology
prevention
clinical care
service delivery and organisation of healthcare (including implementation science)
global health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


