{"title":"局部晚期直肠癌患者卡培他滨加奥沙利铂新辅助化疗后全切除或肿瘤特异性直肠系膜切除伴或不伴侧盆腔淋巴结清扫的短期结果","authors":"Wataru Sakamoto, Yasuyuki Kanke, Hisashi Onozawa, Hirokazu Okayama, Hisahito Endo, Shotaro Fujita, Motonobu Saito, Zenichiro Saze, Tomoyuki Momma, Koji Kono","doi":"10.5387/fms.2022-07","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The standard strategy in Japan for locally advanced rectal cancer is total mesorectal excision plus adjuvant chemotherapy. However, large tumors significantly restrict pelvic manipulation of the distal side of the tumor during surgery;therefore, from an oncological point of view, it is better to shrink the tumor as much as possible preoperatively to optimize the circumferential resection margin. In recent years, advances in systemic chemotherapy have significantly improved the tumor reduction effect, enabling such drug therapy prior to surgery for locally advanced rectal cancer. We herein retrospectively evaluated the clinical, short-term outcomes of patients treated by neoadjuvant chemotherapy (NAC) using capecitabin and oxaliplatin (CAPOX), focusing on overall safety as well as clinical and pathological staging responses to NAC.</p><p><strong>Methods: </strong>We applied the preoperative chemotherapy protocol to T3-4, any N, M0 or M1a (with resectable metastases) (UICC 8<sup>th</sup>) Ra/Rb rectal cancers. The chemotherapy regimen consisted of four cycles of CAPOX. After NAC, curative intent surgery with total mesorectal excision/tumor-specific mesorectal excision with/without metastasectomy was performed. Adverse effects (AEs) and compliance with NAC, surgical complications, clinical and pathological staging were evaluated. All patients undergoing the protocol between January 2017 and June 2021 at Fukushima Medical University were enrolled.</p><p><strong>Results: </strong>Twenty cases were enrolled. No severe AEs were observed either preoperatively or perioperatively. Preoperative assessment of NAC showed no cases of progressive disease (PD). Radical resection was achieved in all cases. Histological therapeutic grading after NAC revealed one grade 3, four grade 2, three grade 1b, eleven grade 1a and one grade 0 among all cases.</p><p><strong>Conclusion: </strong>This study suggests that NAC for locally advanced rectal cancer is likely to be acceptable because there were no severe AEs pre- or perioperatively, radical resection was achieved in all cases, and there were no cases of PD.</p>","PeriodicalId":44831,"journal":{"name":"Fukushima Journal of Medical Science","volume":null,"pages":null},"PeriodicalIF":0.7000,"publicationDate":"2022-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/5b/2185-4610-68-089.PMC9493336.pdf","citationCount":"0","resultStr":"{\"title\":\"Short-term outcomes of neoadjuvant chemotherapy with capecitabine plus oxaliplatin for patients with locally advanced rectal cancer followed by total or tumor-specific mesorectal excision with or without lateral pelvic lymph node dissection.\",\"authors\":\"Wataru Sakamoto, Yasuyuki Kanke, Hisashi Onozawa, Hirokazu Okayama, Hisahito Endo, Shotaro Fujita, Motonobu Saito, Zenichiro Saze, Tomoyuki Momma, Koji Kono\",\"doi\":\"10.5387/fms.2022-07\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The standard strategy in Japan for locally advanced rectal cancer is total mesorectal excision plus adjuvant chemotherapy. However, large tumors significantly restrict pelvic manipulation of the distal side of the tumor during surgery;therefore, from an oncological point of view, it is better to shrink the tumor as much as possible preoperatively to optimize the circumferential resection margin. In recent years, advances in systemic chemotherapy have significantly improved the tumor reduction effect, enabling such drug therapy prior to surgery for locally advanced rectal cancer. We herein retrospectively evaluated the clinical, short-term outcomes of patients treated by neoadjuvant chemotherapy (NAC) using capecitabin and oxaliplatin (CAPOX), focusing on overall safety as well as clinical and pathological staging responses to NAC.</p><p><strong>Methods: </strong>We applied the preoperative chemotherapy protocol to T3-4, any N, M0 or M1a (with resectable metastases) (UICC 8<sup>th</sup>) Ra/Rb rectal cancers. The chemotherapy regimen consisted of four cycles of CAPOX. After NAC, curative intent surgery with total mesorectal excision/tumor-specific mesorectal excision with/without metastasectomy was performed. Adverse effects (AEs) and compliance with NAC, surgical complications, clinical and pathological staging were evaluated. All patients undergoing the protocol between January 2017 and June 2021 at Fukushima Medical University were enrolled.</p><p><strong>Results: </strong>Twenty cases were enrolled. No severe AEs were observed either preoperatively or perioperatively. Preoperative assessment of NAC showed no cases of progressive disease (PD). Radical resection was achieved in all cases. Histological therapeutic grading after NAC revealed one grade 3, four grade 2, three grade 1b, eleven grade 1a and one grade 0 among all cases.</p><p><strong>Conclusion: </strong>This study suggests that NAC for locally advanced rectal cancer is likely to be acceptable because there were no severe AEs pre- or perioperatively, radical resection was achieved in all cases, and there were no cases of PD.</p>\",\"PeriodicalId\":44831,\"journal\":{\"name\":\"Fukushima Journal of Medical Science\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-08-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/5b/2185-4610-68-089.PMC9493336.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Fukushima Journal of Medical Science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5387/fms.2022-07\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/6/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fukushima Journal of Medical Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5387/fms.2022-07","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Short-term outcomes of neoadjuvant chemotherapy with capecitabine plus oxaliplatin for patients with locally advanced rectal cancer followed by total or tumor-specific mesorectal excision with or without lateral pelvic lymph node dissection.
Background: The standard strategy in Japan for locally advanced rectal cancer is total mesorectal excision plus adjuvant chemotherapy. However, large tumors significantly restrict pelvic manipulation of the distal side of the tumor during surgery;therefore, from an oncological point of view, it is better to shrink the tumor as much as possible preoperatively to optimize the circumferential resection margin. In recent years, advances in systemic chemotherapy have significantly improved the tumor reduction effect, enabling such drug therapy prior to surgery for locally advanced rectal cancer. We herein retrospectively evaluated the clinical, short-term outcomes of patients treated by neoadjuvant chemotherapy (NAC) using capecitabin and oxaliplatin (CAPOX), focusing on overall safety as well as clinical and pathological staging responses to NAC.
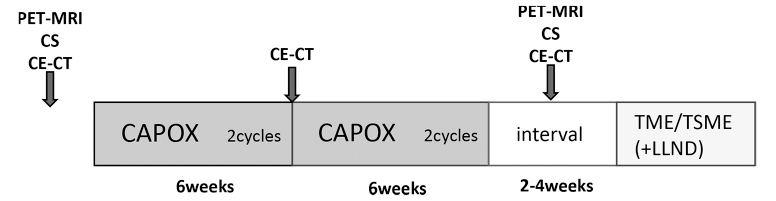
Methods: We applied the preoperative chemotherapy protocol to T3-4, any N, M0 or M1a (with resectable metastases) (UICC 8th) Ra/Rb rectal cancers. The chemotherapy regimen consisted of four cycles of CAPOX. After NAC, curative intent surgery with total mesorectal excision/tumor-specific mesorectal excision with/without metastasectomy was performed. Adverse effects (AEs) and compliance with NAC, surgical complications, clinical and pathological staging were evaluated. All patients undergoing the protocol between January 2017 and June 2021 at Fukushima Medical University were enrolled.
Results: Twenty cases were enrolled. No severe AEs were observed either preoperatively or perioperatively. Preoperative assessment of NAC showed no cases of progressive disease (PD). Radical resection was achieved in all cases. Histological therapeutic grading after NAC revealed one grade 3, four grade 2, three grade 1b, eleven grade 1a and one grade 0 among all cases.
Conclusion: This study suggests that NAC for locally advanced rectal cancer is likely to be acceptable because there were no severe AEs pre- or perioperatively, radical resection was achieved in all cases, and there were no cases of PD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


