Farah Ghieh, Anne-Laure Barbotin, Julie Prasivoravong, Sophie Ferlicot, Béatrice Mandon-Pepin, Joanne Fortemps, Henri-Jean Garchon, Valérie Serazin, Clara Leroy, François Marcelli, François Vialard
{"title":"无精子症和互易位:应该推荐全外显子组测序吗?","authors":"Farah Ghieh, Anne-Laure Barbotin, Julie Prasivoravong, Sophie Ferlicot, Béatrice Mandon-Pepin, Joanne Fortemps, Henri-Jean Garchon, Valérie Serazin, Clara Leroy, François Marcelli, François Vialard","doi":"10.1186/s12610-021-00145-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although chromosome rearrangements are responsible for spermatogenesis failure, their impact depends greatly on the chromosomes involved. At present, karyotyping and Y chromosome microdeletion screening are the first-line genetic tests for patients with non-obstructive azoospermia. Although it is generally acknowledged that X or Y chromosome rearrangements lead to meiotic arrest and thus rule out any chance of sperm retrieval after a testicular biopsy, we currently lack markers for the likelihood of testicular sperm extraction (TESE) in patients with other chromosome rearrangements.</p><p><strong>Results: </strong>We investigated the use of a single nucleotide polymorphism comparative genome hybridization array (SNP-CGH) and whole-exome sequencing (WES) for two patients with non-obstructive azoospermia and testicular meiotic arrest, a reciprocal translocation: t(X;21) and t(20;22), and an unsuccessful TESE. No additional gene defects were identified for the t(X;21) carrier - suggesting that t(X;21) alone damages spermatogenesis. In contrast, the highly consanguineous t(20;22) carrier had two deleterious homozygous variants in the TMPRSS9 gene; these might have contributed to testicular meiotic arrest. Genetic defect was confirmed with Sanger sequencing and immunohistochemical assessments on testicular tissue sections.</p><p><strong>Conclusions: </strong>Firstly, TMPRSS9 gene defects might impact spermatogenesis. Secondly, as a function of the chromosome breakpoints for azoospermic patients with chromosome rearrangements, provision of the best possible genetic counselling means that genetic testing should not be limited to karyotyping. Given the risks associated with TESE, it is essential to perform WES - especially for consanguineous patients.</p>","PeriodicalId":8730,"journal":{"name":"Basic and Clinical Andrology","volume":null,"pages":null},"PeriodicalIF":2.4000,"publicationDate":"2021-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8582189/pdf/","citationCount":"4","resultStr":"{\"title\":\"Azoospermia and reciprocal translocations: should whole-exome sequencing be recommended?\",\"authors\":\"Farah Ghieh, Anne-Laure Barbotin, Julie Prasivoravong, Sophie Ferlicot, Béatrice Mandon-Pepin, Joanne Fortemps, Henri-Jean Garchon, Valérie Serazin, Clara Leroy, François Marcelli, François Vialard\",\"doi\":\"10.1186/s12610-021-00145-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Although chromosome rearrangements are responsible for spermatogenesis failure, their impact depends greatly on the chromosomes involved. At present, karyotyping and Y chromosome microdeletion screening are the first-line genetic tests for patients with non-obstructive azoospermia. Although it is generally acknowledged that X or Y chromosome rearrangements lead to meiotic arrest and thus rule out any chance of sperm retrieval after a testicular biopsy, we currently lack markers for the likelihood of testicular sperm extraction (TESE) in patients with other chromosome rearrangements.</p><p><strong>Results: </strong>We investigated the use of a single nucleotide polymorphism comparative genome hybridization array (SNP-CGH) and whole-exome sequencing (WES) for two patients with non-obstructive azoospermia and testicular meiotic arrest, a reciprocal translocation: t(X;21) and t(20;22), and an unsuccessful TESE. No additional gene defects were identified for the t(X;21) carrier - suggesting that t(X;21) alone damages spermatogenesis. In contrast, the highly consanguineous t(20;22) carrier had two deleterious homozygous variants in the TMPRSS9 gene; these might have contributed to testicular meiotic arrest. Genetic defect was confirmed with Sanger sequencing and immunohistochemical assessments on testicular tissue sections.</p><p><strong>Conclusions: </strong>Firstly, TMPRSS9 gene defects might impact spermatogenesis. Secondly, as a function of the chromosome breakpoints for azoospermic patients with chromosome rearrangements, provision of the best possible genetic counselling means that genetic testing should not be limited to karyotyping. Given the risks associated with TESE, it is essential to perform WES - especially for consanguineous patients.</p>\",\"PeriodicalId\":8730,\"journal\":{\"name\":\"Basic and Clinical Andrology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2021-11-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8582189/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Basic and Clinical Andrology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12610-021-00145-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANDROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Basic and Clinical Andrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12610-021-00145-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANDROLOGY","Score":null,"Total":0}
Azoospermia and reciprocal translocations: should whole-exome sequencing be recommended?
Background: Although chromosome rearrangements are responsible for spermatogenesis failure, their impact depends greatly on the chromosomes involved. At present, karyotyping and Y chromosome microdeletion screening are the first-line genetic tests for patients with non-obstructive azoospermia. Although it is generally acknowledged that X or Y chromosome rearrangements lead to meiotic arrest and thus rule out any chance of sperm retrieval after a testicular biopsy, we currently lack markers for the likelihood of testicular sperm extraction (TESE) in patients with other chromosome rearrangements.
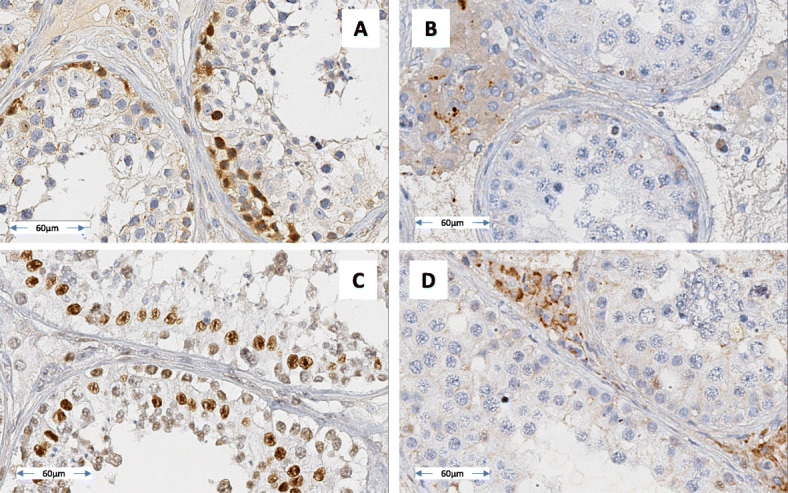
Results: We investigated the use of a single nucleotide polymorphism comparative genome hybridization array (SNP-CGH) and whole-exome sequencing (WES) for two patients with non-obstructive azoospermia and testicular meiotic arrest, a reciprocal translocation: t(X;21) and t(20;22), and an unsuccessful TESE. No additional gene defects were identified for the t(X;21) carrier - suggesting that t(X;21) alone damages spermatogenesis. In contrast, the highly consanguineous t(20;22) carrier had two deleterious homozygous variants in the TMPRSS9 gene; these might have contributed to testicular meiotic arrest. Genetic defect was confirmed with Sanger sequencing and immunohistochemical assessments on testicular tissue sections.
Conclusions: Firstly, TMPRSS9 gene defects might impact spermatogenesis. Secondly, as a function of the chromosome breakpoints for azoospermic patients with chromosome rearrangements, provision of the best possible genetic counselling means that genetic testing should not be limited to karyotyping. Given the risks associated with TESE, it is essential to perform WES - especially for consanguineous patients.
期刊介绍:
Basic and Clinical Andrology is an open access journal in the domain of andrology covering all aspects of male reproductive and sexual health in both human and animal models. The journal aims to bring to light the various clinical advancements and research developments in andrology from the international community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


