Bandar M Faqihi, Samuel P Trethewey, Julien Morlet, Dhruv Parekh, Alice M Turner
{"title":"双水平气道正压通气治疗非copd急性高碳酸血症性呼吸衰竭:一项系统综述和荟萃分析。","authors":"Bandar M Faqihi, Samuel P Trethewey, Julien Morlet, Dhruv Parekh, Alice M Turner","doi":"10.4103/atm.atm_683_20","DOIUrl":null,"url":null,"abstract":"<p><p>The effectiveness of bi-level positive airway pressure (BiPAP) in patients with acute hypercapnic respiratory failure (AHRF) due to etiologies other than chronic obstructive pulmonary disease (COPD) is unclear. To systematically review the evidence regarding the effectiveness of BiPAP in non-COPD patients with AHRF. The Cochrane Library, MEDLINE, EMBASE, and CINAHL Plus were searched according to prespecified criteria (PROSPERO-CRD42018089875). Randomized controlled trials (RCTs) assessing the effectiveness of BiPAP versus continuous positive airway pressure (CPAP), invasive mechanical ventilation, or O<sub>2</sub> therapy in adults with non-COPD AHRF were included. The primary outcomes of interest were the rate of endotracheal intubation (ETI) and mortality. Risk-of-bias assessment was performed, and data were synthesized and meta-analyzed where appropriate. Two thousand four hundred and eighty-five records were identified after removing duplicates. Eighty-eight articles were identified for full-text assessment, of which 82 articles were excluded. Six studies, of generally low or uncertain risk-of-bias, were included involving 320 participants with acute cardiogenic pulmonary edema (ACPO) and solid tumors. No significant differences were seen between BiPAP ventilation and CPAP with regard to the rate of progression to ETI (risk ratio [RR] = 1.49, 95% confidence interval [CI], 0.63-3.62, <i>P</i> = 0.37) and in-hospital mortality rate (RR = 0.71, 95% CI, 0.25-1.99, <i>P</i> = 0.51) in patients with AHRF due to ACPO. The efficacy of BiPAP appears similar to CPAP in reducing the rates of ETI and mortality in patients with AHRF due to ACPO. Further research on other non-COPD conditions which commonly cause AHRF such as obesity hypoventilation syndrome is needed.</p>","PeriodicalId":50760,"journal":{"name":"Annals of Thoracic Medicine","volume":"16 4","pages":"306-322"},"PeriodicalIF":2.1000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/bf/ATM-16-306.PMC8588943.pdf","citationCount":"2","resultStr":"{\"title\":\"Bilevel positive airway pressure ventilation for non-COPD acute hypercapnic respiratory failure patients: A systematic review and meta-analysis.\",\"authors\":\"Bandar M Faqihi, Samuel P Trethewey, Julien Morlet, Dhruv Parekh, Alice M Turner\",\"doi\":\"10.4103/atm.atm_683_20\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The effectiveness of bi-level positive airway pressure (BiPAP) in patients with acute hypercapnic respiratory failure (AHRF) due to etiologies other than chronic obstructive pulmonary disease (COPD) is unclear. To systematically review the evidence regarding the effectiveness of BiPAP in non-COPD patients with AHRF. The Cochrane Library, MEDLINE, EMBASE, and CINAHL Plus were searched according to prespecified criteria (PROSPERO-CRD42018089875). Randomized controlled trials (RCTs) assessing the effectiveness of BiPAP versus continuous positive airway pressure (CPAP), invasive mechanical ventilation, or O<sub>2</sub> therapy in adults with non-COPD AHRF were included. The primary outcomes of interest were the rate of endotracheal intubation (ETI) and mortality. Risk-of-bias assessment was performed, and data were synthesized and meta-analyzed where appropriate. Two thousand four hundred and eighty-five records were identified after removing duplicates. Eighty-eight articles were identified for full-text assessment, of which 82 articles were excluded. Six studies, of generally low or uncertain risk-of-bias, were included involving 320 participants with acute cardiogenic pulmonary edema (ACPO) and solid tumors. No significant differences were seen between BiPAP ventilation and CPAP with regard to the rate of progression to ETI (risk ratio [RR] = 1.49, 95% confidence interval [CI], 0.63-3.62, <i>P</i> = 0.37) and in-hospital mortality rate (RR = 0.71, 95% CI, 0.25-1.99, <i>P</i> = 0.51) in patients with AHRF due to ACPO. The efficacy of BiPAP appears similar to CPAP in reducing the rates of ETI and mortality in patients with AHRF due to ACPO. Further research on other non-COPD conditions which commonly cause AHRF such as obesity hypoventilation syndrome is needed.</p>\",\"PeriodicalId\":50760,\"journal\":{\"name\":\"Annals of Thoracic Medicine\",\"volume\":\"16 4\",\"pages\":\"306-322\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2021-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/bf/ATM-16-306.PMC8588943.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4103/atm.atm_683_20\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/10/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/atm.atm_683_20","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
摘要
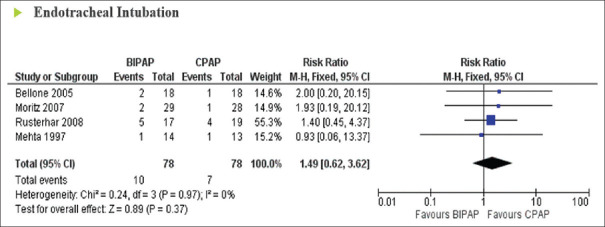
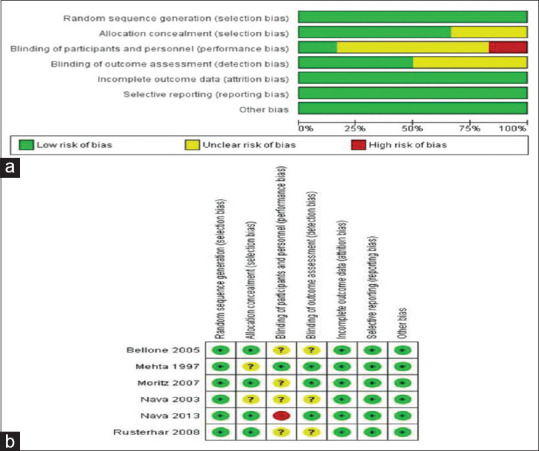
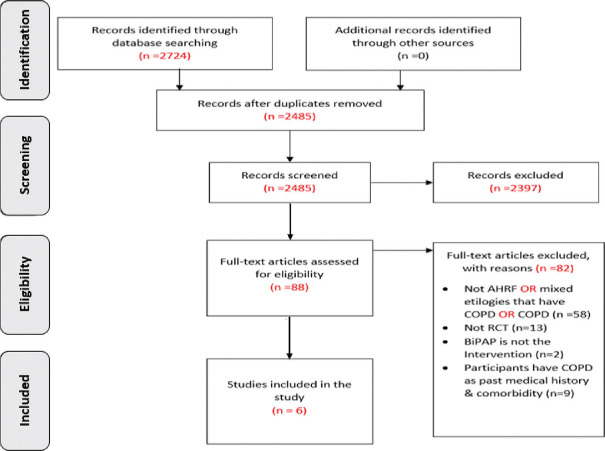
双水平气道正压通气(BiPAP)治疗非慢性阻塞性肺疾病(COPD)所致急性高碳酸血症性呼吸衰竭(AHRF)的有效性尚不清楚。系统回顾BiPAP治疗非copd AHRF患者有效性的证据。根据预设标准检索Cochrane Library、MEDLINE、EMBASE和CINAHL Plus (PROSPERO-CRD42018089875)。随机对照试验(rct)评估了BiPAP与持续气道正压通气(CPAP)、有创机械通气或氧气治疗在成人非copd AHRF中的有效性。研究的主要结局是气管插管率(ETI)和死亡率。进行偏倚风险评估,并在适当的地方对数据进行综合和荟萃分析。在删除重复项后,确定了两千四百八十五条记录。确定88篇文章进行全文评估,其中82篇文章被排除。6项偏倚风险一般较低或不确定的研究纳入了320名急性心源性肺水肿(ACPO)和实体瘤患者。在ACPO所致AHRF患者的ETI进展率(风险比[RR] = 1.49, 95%可信区间[CI], 0.63-3.62, P = 0.37)和住院死亡率(RR = 0.71, 95% CI, 0.25-1.99, P = 0.51)方面,BiPAP通气与CPAP通气无显著差异。BiPAP在降低ACPO所致AHRF患者ETI和死亡率方面的疗效与CPAP相似。其他非慢性阻塞性肺疾病如肥胖低通气综合征等通常引起AHRF的情况需要进一步研究。
Bilevel positive airway pressure ventilation for non-COPD acute hypercapnic respiratory failure patients: A systematic review and meta-analysis.
The effectiveness of bi-level positive airway pressure (BiPAP) in patients with acute hypercapnic respiratory failure (AHRF) due to etiologies other than chronic obstructive pulmonary disease (COPD) is unclear. To systematically review the evidence regarding the effectiveness of BiPAP in non-COPD patients with AHRF. The Cochrane Library, MEDLINE, EMBASE, and CINAHL Plus were searched according to prespecified criteria (PROSPERO-CRD42018089875). Randomized controlled trials (RCTs) assessing the effectiveness of BiPAP versus continuous positive airway pressure (CPAP), invasive mechanical ventilation, or O2 therapy in adults with non-COPD AHRF were included. The primary outcomes of interest were the rate of endotracheal intubation (ETI) and mortality. Risk-of-bias assessment was performed, and data were synthesized and meta-analyzed where appropriate. Two thousand four hundred and eighty-five records were identified after removing duplicates. Eighty-eight articles were identified for full-text assessment, of which 82 articles were excluded. Six studies, of generally low or uncertain risk-of-bias, were included involving 320 participants with acute cardiogenic pulmonary edema (ACPO) and solid tumors. No significant differences were seen between BiPAP ventilation and CPAP with regard to the rate of progression to ETI (risk ratio [RR] = 1.49, 95% confidence interval [CI], 0.63-3.62, P = 0.37) and in-hospital mortality rate (RR = 0.71, 95% CI, 0.25-1.99, P = 0.51) in patients with AHRF due to ACPO. The efficacy of BiPAP appears similar to CPAP in reducing the rates of ETI and mortality in patients with AHRF due to ACPO. Further research on other non-COPD conditions which commonly cause AHRF such as obesity hypoventilation syndrome is needed.
期刊介绍:
The journal will cover studies related to multidisciplinary specialties of chest medicine, such as adult and pediatrics pulmonology, thoracic surgery, critical care medicine, respiratory care, transplantation, sleep medicine, related basic medical sciences, and more. The journal also features basic science, special reports, case reports, board review , and more. Editorials and communications to the editor that explore controversial issues and encourage further discussion by physicians dealing with chest medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


