{"title":"腹主动脉完全闭塞:在老年人中仍然是一个致命的事件。","authors":"Gonçalo José Pereira Carneiro, Carla Martins","doi":"10.22551/2021.32.0803.10184","DOIUrl":null,"url":null,"abstract":"<p><p>Total occlusion of the abdominal aorta is an uncommon but potentially devastating event. Clinical symptoms are usually sudden and may vary depending on the level of the aortic occlusion. Associated morbidity and mortality remain substantial with high rates of limb loss, acute renal failure, rhabdomyolysis, and death. We report a case of a bedridden 91-year-old woman with history of hypertension, hyperlipidemia, anemia and dementia, carried to the emergency department because of bilateral lower limb pallor. She had been at the same department the week before because of the same problems and high blood pressure (BP), but had been discharged after administration of hypotensive drugs and a short period of observation. No attention was paid to those perfusion alterations, or the global picture at all. The physical examination revealed cooling of the lower limbs and significant BP differential between upper and lower limbs (ankle-brachial index of 0.173), leading to the suspicion of bilateral acute limb ischemia. Abdominal, pelvic and lower limb CT was conducted, revealing calcification and important atheromatosis of the thoracic-abdominal aorta and a mural thrombus beginning above the origin of the celiac trunk, with complete occlusion below the origin of the renal arteries. After discussion with Vascular Surgery Department, given the advanced age, known co-morbidities and the timing of diagnosis, the patient was considered not eligible for revascularization surgery and comfort measures were honored. This case highlights the importance of stablishing a timely and correct diagnosis, even in the very elderly, emphasizing that they too benefit from secondary and tertiary prophylaxis, in order to prevent devastating outcomes as this.</p>","PeriodicalId":72274,"journal":{"name":"Archive of clinical cases","volume":"8 3","pages":"42-45"},"PeriodicalIF":0.8000,"publicationDate":"2021-12-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/12/acc-08-03-42.PMC8717000.pdf","citationCount":"0","resultStr":"{\"title\":\"Total occlusion of abdominal aorta: still a deadly event in the very elderly.\",\"authors\":\"Gonçalo José Pereira Carneiro, Carla Martins\",\"doi\":\"10.22551/2021.32.0803.10184\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Total occlusion of the abdominal aorta is an uncommon but potentially devastating event. Clinical symptoms are usually sudden and may vary depending on the level of the aortic occlusion. Associated morbidity and mortality remain substantial with high rates of limb loss, acute renal failure, rhabdomyolysis, and death. We report a case of a bedridden 91-year-old woman with history of hypertension, hyperlipidemia, anemia and dementia, carried to the emergency department because of bilateral lower limb pallor. She had been at the same department the week before because of the same problems and high blood pressure (BP), but had been discharged after administration of hypotensive drugs and a short period of observation. No attention was paid to those perfusion alterations, or the global picture at all. The physical examination revealed cooling of the lower limbs and significant BP differential between upper and lower limbs (ankle-brachial index of 0.173), leading to the suspicion of bilateral acute limb ischemia. Abdominal, pelvic and lower limb CT was conducted, revealing calcification and important atheromatosis of the thoracic-abdominal aorta and a mural thrombus beginning above the origin of the celiac trunk, with complete occlusion below the origin of the renal arteries. After discussion with Vascular Surgery Department, given the advanced age, known co-morbidities and the timing of diagnosis, the patient was considered not eligible for revascularization surgery and comfort measures were honored. This case highlights the importance of stablishing a timely and correct diagnosis, even in the very elderly, emphasizing that they too benefit from secondary and tertiary prophylaxis, in order to prevent devastating outcomes as this.</p>\",\"PeriodicalId\":72274,\"journal\":{\"name\":\"Archive of clinical cases\",\"volume\":\"8 3\",\"pages\":\"42-45\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2021-12-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/12/acc-08-03-42.PMC8717000.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archive of clinical cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22551/2021.32.0803.10184\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archive of clinical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22551/2021.32.0803.10184","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Total occlusion of abdominal aorta: still a deadly event in the very elderly.
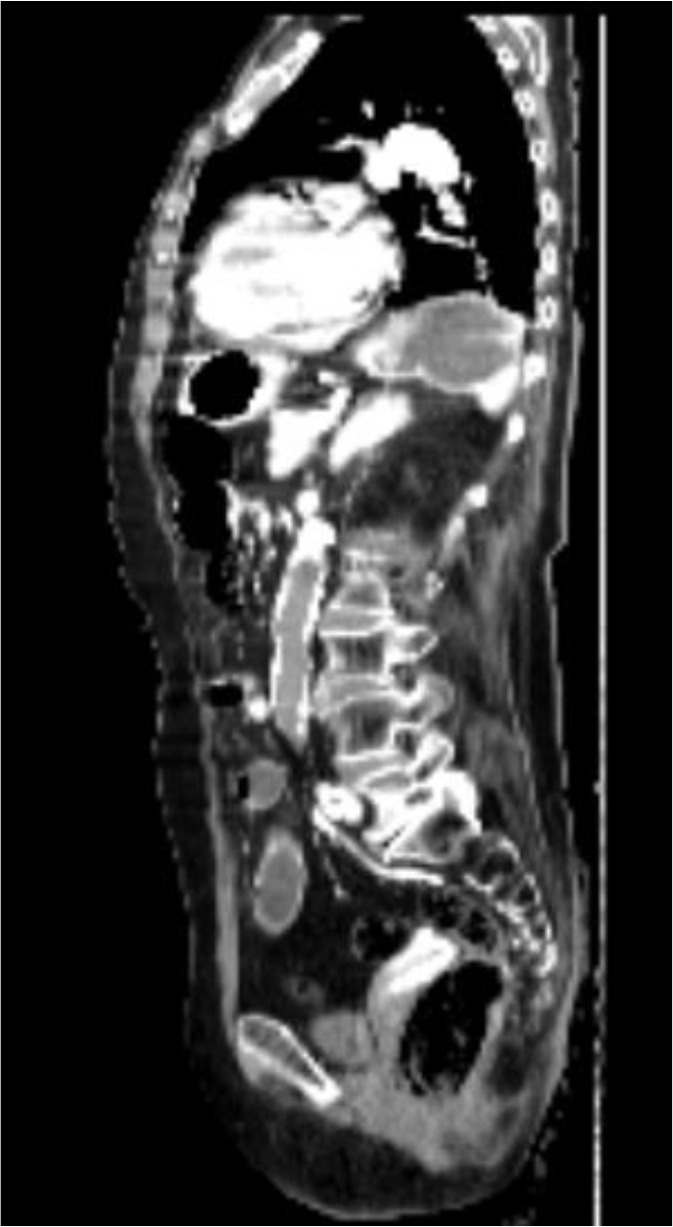
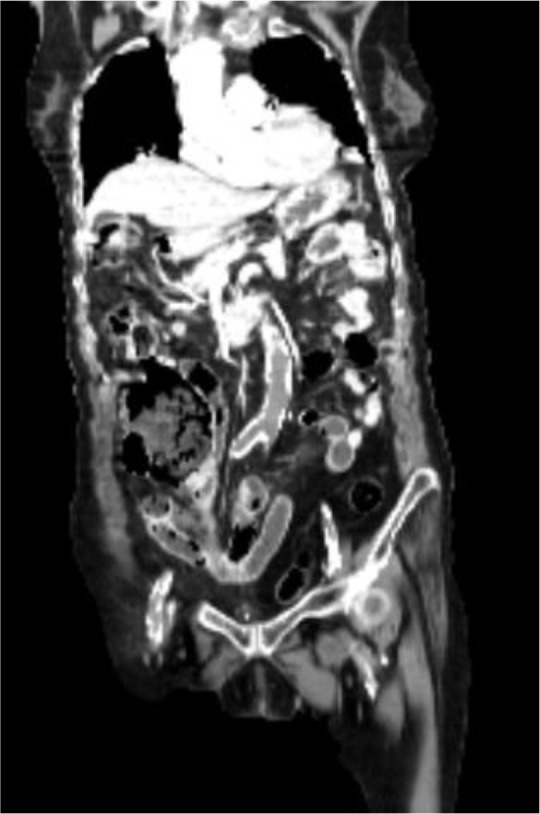
Total occlusion of the abdominal aorta is an uncommon but potentially devastating event. Clinical symptoms are usually sudden and may vary depending on the level of the aortic occlusion. Associated morbidity and mortality remain substantial with high rates of limb loss, acute renal failure, rhabdomyolysis, and death. We report a case of a bedridden 91-year-old woman with history of hypertension, hyperlipidemia, anemia and dementia, carried to the emergency department because of bilateral lower limb pallor. She had been at the same department the week before because of the same problems and high blood pressure (BP), but had been discharged after administration of hypotensive drugs and a short period of observation. No attention was paid to those perfusion alterations, or the global picture at all. The physical examination revealed cooling of the lower limbs and significant BP differential between upper and lower limbs (ankle-brachial index of 0.173), leading to the suspicion of bilateral acute limb ischemia. Abdominal, pelvic and lower limb CT was conducted, revealing calcification and important atheromatosis of the thoracic-abdominal aorta and a mural thrombus beginning above the origin of the celiac trunk, with complete occlusion below the origin of the renal arteries. After discussion with Vascular Surgery Department, given the advanced age, known co-morbidities and the timing of diagnosis, the patient was considered not eligible for revascularization surgery and comfort measures were honored. This case highlights the importance of stablishing a timely and correct diagnosis, even in the very elderly, emphasizing that they too benefit from secondary and tertiary prophylaxis, in order to prevent devastating outcomes as this.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


