{"title":"长期随访期间对比度诱发肾病的不良预后。","authors":"Taili Liu, Sang-Rok Lee","doi":"10.4068/cmj.2021.57.3.197","DOIUrl":null,"url":null,"abstract":"<p><p>Contrast-induced nephropathy (CIN) is known to associate with poor prognosis. However, there have been few studies for long-term follow up. The purpose of this study was to know the prognosis of CIN during a 10-year follow up. We retrospectively analyzed 528 patients who underwent coronary angiography in Jeonbuk National University Hospital (South Korea, Jeonju) between Jan 2005 to Dec 2006. We excluded the patients who required regular dialysis before study enrollment. We compared adverse events in the no CIN (group I, n=485, 61.9±11.4 years, male 64.1%) and CIN (group II, n=43, 65.7±11.1 years, male 62.8%). Baseline clinical characteristics and cardiovascular risk factors were not different between the two groups except the post-procedure creatinine level (1.04 mg/dL vs 1.84 mg/dL, p=0.0001). The higher rates of all-cause death were observed in group II at 1-year (3.7% vs 13.9%, log-rank, p=0.001), 5-years (17.9% vs 34.9%, log-rank, p=0.003), and 10-years (25.3% vs 48.8%, log-rank, p=0.000). MACE was higher in group II at 1-year (3.9% vs 11.6%, log-rank, p=0.013), 5-years (6.8% vs 20.9%, log-rank, p=0.000) and 10-years (13.4% vs 27.9%, log-rank, p=0.000). In addition, CIN was an independent predictor for 10-year MACE (adjusted HR 3.432, 95% CI 1.314-8.965, p=0.012) after propensity score matching. The worse prognosis of CIN was continuously observed after the 10-year follow-up. Our data suggests that it is worthwhile to prevent the appearance of CIN in order to improve longterm results.</p>","PeriodicalId":10307,"journal":{"name":"Chonnam Medical Journal","volume":"57 3","pages":"197-203"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/27/86/cmj-57-197.PMC8485089.pdf","citationCount":"0","resultStr":"{\"title\":\"Poor Prognosis of Contrast-Induced Nephropathy during Long Term Follow Up.\",\"authors\":\"Taili Liu, Sang-Rok Lee\",\"doi\":\"10.4068/cmj.2021.57.3.197\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Contrast-induced nephropathy (CIN) is known to associate with poor prognosis. However, there have been few studies for long-term follow up. The purpose of this study was to know the prognosis of CIN during a 10-year follow up. We retrospectively analyzed 528 patients who underwent coronary angiography in Jeonbuk National University Hospital (South Korea, Jeonju) between Jan 2005 to Dec 2006. We excluded the patients who required regular dialysis before study enrollment. We compared adverse events in the no CIN (group I, n=485, 61.9±11.4 years, male 64.1%) and CIN (group II, n=43, 65.7±11.1 years, male 62.8%). Baseline clinical characteristics and cardiovascular risk factors were not different between the two groups except the post-procedure creatinine level (1.04 mg/dL vs 1.84 mg/dL, p=0.0001). The higher rates of all-cause death were observed in group II at 1-year (3.7% vs 13.9%, log-rank, p=0.001), 5-years (17.9% vs 34.9%, log-rank, p=0.003), and 10-years (25.3% vs 48.8%, log-rank, p=0.000). MACE was higher in group II at 1-year (3.9% vs 11.6%, log-rank, p=0.013), 5-years (6.8% vs 20.9%, log-rank, p=0.000) and 10-years (13.4% vs 27.9%, log-rank, p=0.000). In addition, CIN was an independent predictor for 10-year MACE (adjusted HR 3.432, 95% CI 1.314-8.965, p=0.012) after propensity score matching. The worse prognosis of CIN was continuously observed after the 10-year follow-up. Our data suggests that it is worthwhile to prevent the appearance of CIN in order to improve longterm results.</p>\",\"PeriodicalId\":10307,\"journal\":{\"name\":\"Chonnam Medical Journal\",\"volume\":\"57 3\",\"pages\":\"197-203\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/27/86/cmj-57-197.PMC8485089.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chonnam Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4068/cmj.2021.57.3.197\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/9/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chonnam Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4068/cmj.2021.57.3.197","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
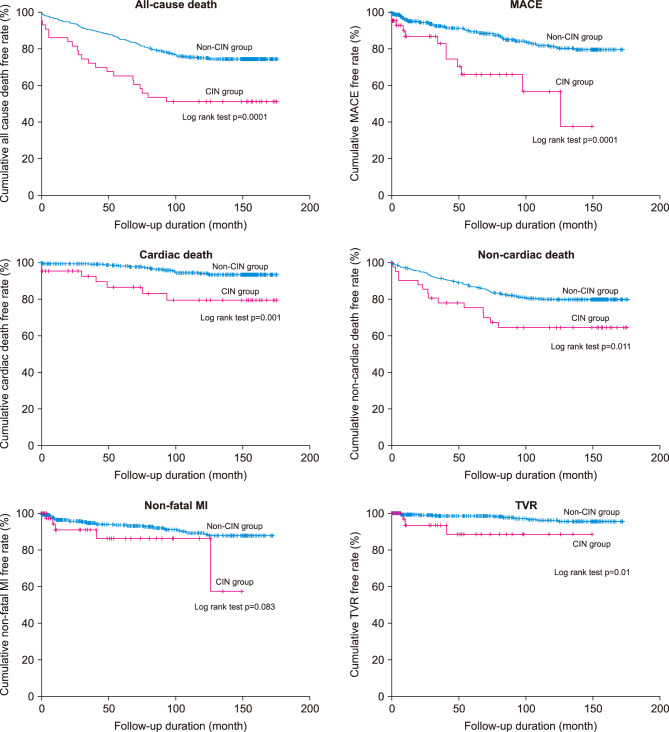
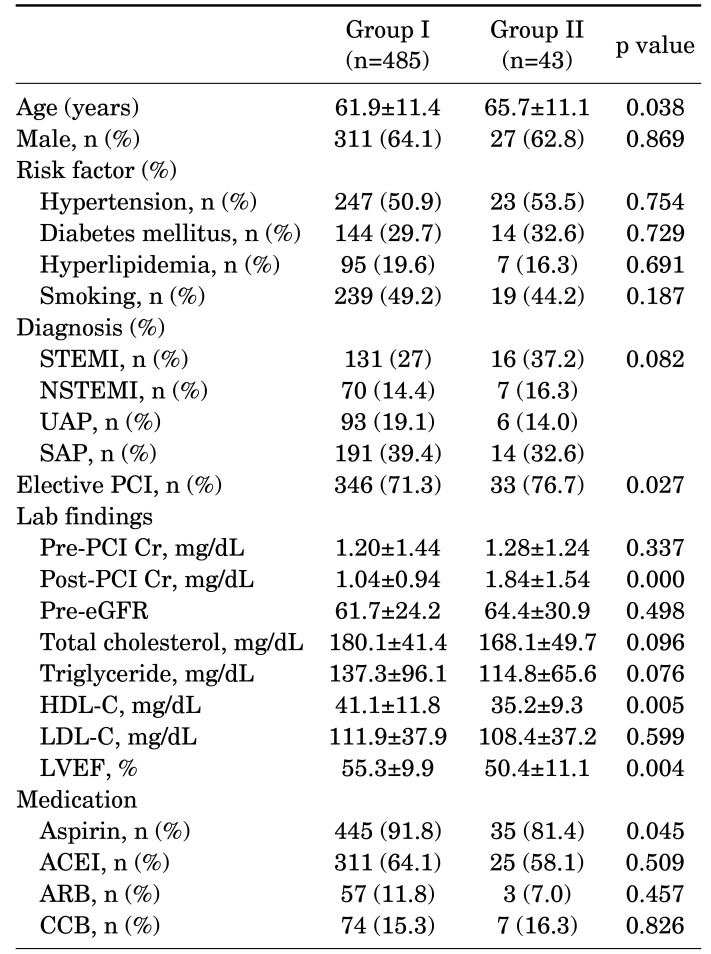
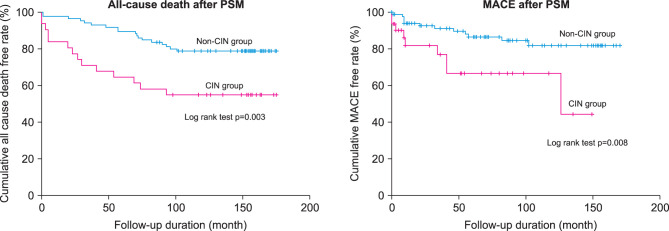
众所周知,造影剂诱发肾病(CIN)与预后不良有关。然而,有关长期随访的研究却很少。本研究的目的是了解 10 年随访期间 CIN 的预后情况。我们对 2005 年 1 月至 2006 年 12 月期间在全北国立大学医院(韩国全州)接受冠状动脉造影术的 528 例患者进行了回顾性分析。我们排除了入组前需要定期透析的患者。我们比较了无 CIN 组(I 组,n=485,61.9±11.4 岁,男性占 64.1%)和 CIN 组(II 组,n=43,65.7±11.1 岁,男性占 62.8%)的不良事件。除术后肌酐水平(1.04 mg/dL vs 1.84 mg/dL,P=0.0001)外,两组的基线临床特征和心血管风险因素无差异。观察到第二组全因死亡率较高,分别为1年(3.7% vs 13.9%,log-rank,p=0.001)、5年(17.9% vs 34.9%,log-rank,p=0.003)和10年(25.3% vs 48.8%,log-rank,p=0.000)。II组患者在1年(3.9% vs 11.6%,log-rank,p=0.013)、5年(6.8% vs 20.9%,log-rank,p=0.000)和10年(13.4% vs 27.9%,log-rank,p=0.000)时的MACE较高。此外,倾向评分匹配后,CIN 是 10 年 MACE 的独立预测因子(调整后 HR 3.432,95% CI 1.314-8.965,p=0.012)。10 年随访后仍可观察到 CIN 预后较差的情况。我们的数据表明,为了改善长期效果,值得预防CIN的出现。
Poor Prognosis of Contrast-Induced Nephropathy during Long Term Follow Up.
Contrast-induced nephropathy (CIN) is known to associate with poor prognosis. However, there have been few studies for long-term follow up. The purpose of this study was to know the prognosis of CIN during a 10-year follow up. We retrospectively analyzed 528 patients who underwent coronary angiography in Jeonbuk National University Hospital (South Korea, Jeonju) between Jan 2005 to Dec 2006. We excluded the patients who required regular dialysis before study enrollment. We compared adverse events in the no CIN (group I, n=485, 61.9±11.4 years, male 64.1%) and CIN (group II, n=43, 65.7±11.1 years, male 62.8%). Baseline clinical characteristics and cardiovascular risk factors were not different between the two groups except the post-procedure creatinine level (1.04 mg/dL vs 1.84 mg/dL, p=0.0001). The higher rates of all-cause death were observed in group II at 1-year (3.7% vs 13.9%, log-rank, p=0.001), 5-years (17.9% vs 34.9%, log-rank, p=0.003), and 10-years (25.3% vs 48.8%, log-rank, p=0.000). MACE was higher in group II at 1-year (3.9% vs 11.6%, log-rank, p=0.013), 5-years (6.8% vs 20.9%, log-rank, p=0.000) and 10-years (13.4% vs 27.9%, log-rank, p=0.000). In addition, CIN was an independent predictor for 10-year MACE (adjusted HR 3.432, 95% CI 1.314-8.965, p=0.012) after propensity score matching. The worse prognosis of CIN was continuously observed after the 10-year follow-up. Our data suggests that it is worthwhile to prevent the appearance of CIN in order to improve longterm results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


