{"title":"预测医院诊断编码:价格激励的个体水平效应。","authors":"Kjartan Sarheim Anthun","doi":"10.1007/s10754-021-09314-5","DOIUrl":null,"url":null,"abstract":"<p><p>The purpose of this paper is to test if implicit price incentives influence the diagnostic coding of hospital discharges. We estimate if the probability of being coded as a complicated patient was related to a specific price incentive. This paper tests empirically if upcoding can be linked to shifts in patient composition through proxy measures such as age composition, length of stay, readmission rates, mortality- and morbidity of patients. Data about inpatient episodes in Norway in all specialized hospitals in the years 1999-2012 were collected, N = 11 065 330. We examined incentives present in part of the hospital funding system. First, we analyse trends in the proxy measures of diagnostic upcoding: can hospital behavioural changes be seen over time with regards to age composition, readmission rates, length of stay, comorbidity and mortality? Secondly, we examine specific patient groups to see if variations in the price incentive are related to probability of being coded as complicated. In the first years (1999-2003) there was an observed increase in the share of episodes coded as complicated, while the level has become more stable in the years 2004-2012. The analysis showed some indications of upcoding. However, we found no evidence of widespread upcoding fuelled by implicit price incentive, as other issues such as patient characteristics seem to be more important than the price differences. This study adds to previous research by testing individual level predictions. The added value of such analysis is to have better case mix control. We observe the presence of price effects even at individual level.</p>","PeriodicalId":44403,"journal":{"name":"International Journal of Health Economics and Management","volume":"22 2","pages":"129-146"},"PeriodicalIF":1.7000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9090893/pdf/","citationCount":"2","resultStr":"{\"title\":\"Predicting diagnostic coding in hospitals: individual level effects of price incentives.\",\"authors\":\"Kjartan Sarheim Anthun\",\"doi\":\"10.1007/s10754-021-09314-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The purpose of this paper is to test if implicit price incentives influence the diagnostic coding of hospital discharges. We estimate if the probability of being coded as a complicated patient was related to a specific price incentive. This paper tests empirically if upcoding can be linked to shifts in patient composition through proxy measures such as age composition, length of stay, readmission rates, mortality- and morbidity of patients. Data about inpatient episodes in Norway in all specialized hospitals in the years 1999-2012 were collected, N = 11 065 330. We examined incentives present in part of the hospital funding system. First, we analyse trends in the proxy measures of diagnostic upcoding: can hospital behavioural changes be seen over time with regards to age composition, readmission rates, length of stay, comorbidity and mortality? Secondly, we examine specific patient groups to see if variations in the price incentive are related to probability of being coded as complicated. In the first years (1999-2003) there was an observed increase in the share of episodes coded as complicated, while the level has become more stable in the years 2004-2012. The analysis showed some indications of upcoding. However, we found no evidence of widespread upcoding fuelled by implicit price incentive, as other issues such as patient characteristics seem to be more important than the price differences. This study adds to previous research by testing individual level predictions. The added value of such analysis is to have better case mix control. We observe the presence of price effects even at individual level.</p>\",\"PeriodicalId\":44403,\"journal\":{\"name\":\"International Journal of Health Economics and Management\",\"volume\":\"22 2\",\"pages\":\"129-146\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2022-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9090893/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Health Economics and Management\",\"FirstCategoryId\":\"96\",\"ListUrlMain\":\"https://doi.org/10.1007/s10754-021-09314-5\",\"RegionNum\":4,\"RegionCategory\":\"经济学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/10/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"BUSINESS, FINANCE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Health Economics and Management","FirstCategoryId":"96","ListUrlMain":"https://doi.org/10.1007/s10754-021-09314-5","RegionNum":4,"RegionCategory":"经济学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/6 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"BUSINESS, FINANCE","Score":null,"Total":0}
Predicting diagnostic coding in hospitals: individual level effects of price incentives.
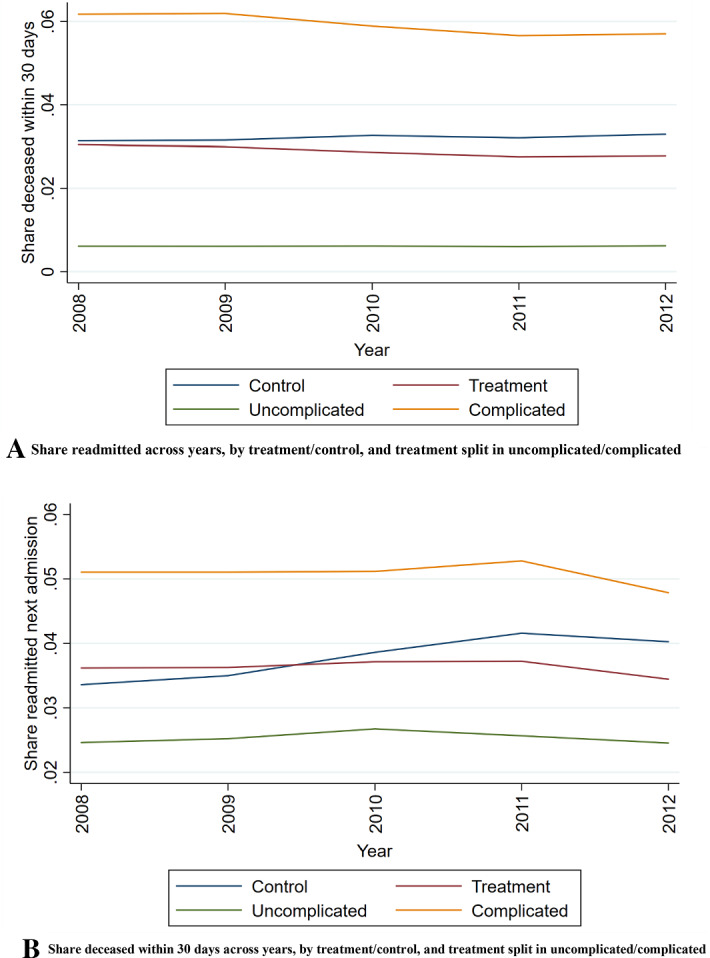
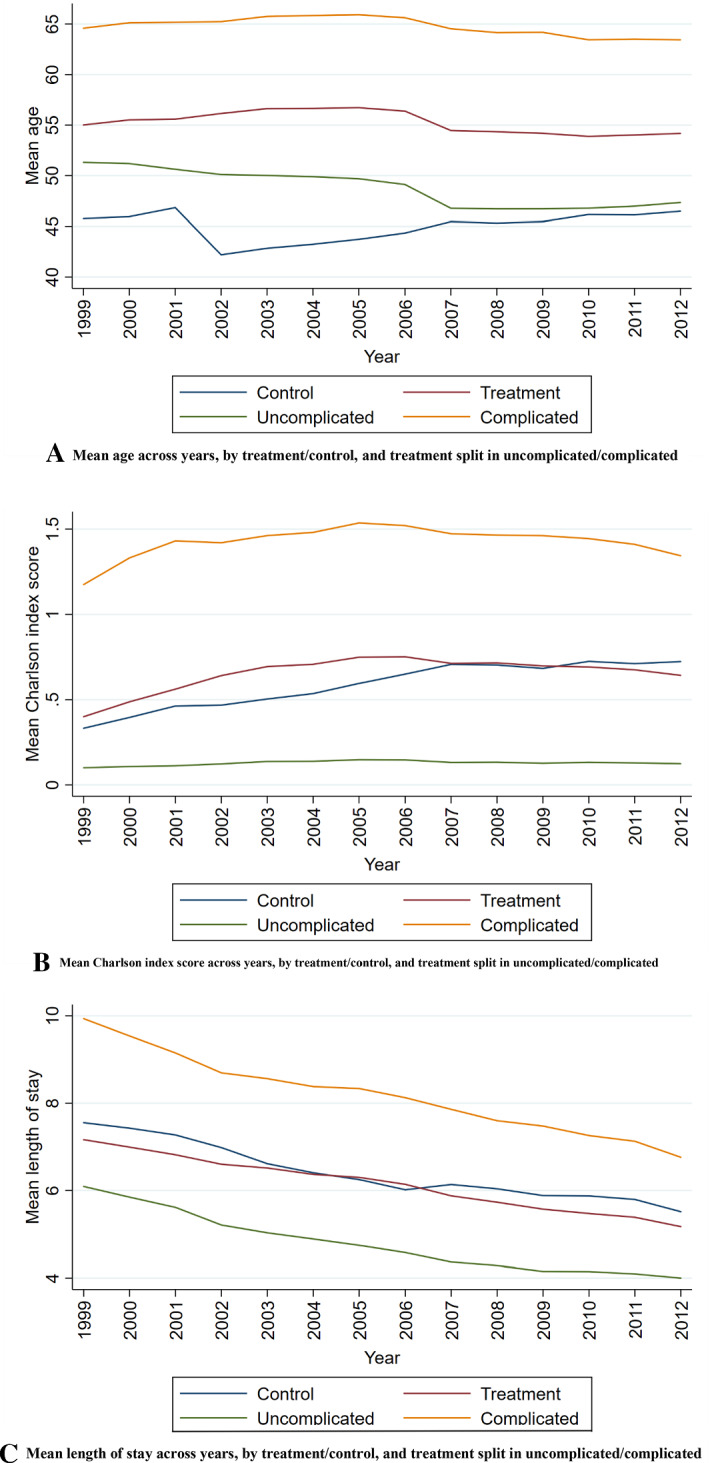
The purpose of this paper is to test if implicit price incentives influence the diagnostic coding of hospital discharges. We estimate if the probability of being coded as a complicated patient was related to a specific price incentive. This paper tests empirically if upcoding can be linked to shifts in patient composition through proxy measures such as age composition, length of stay, readmission rates, mortality- and morbidity of patients. Data about inpatient episodes in Norway in all specialized hospitals in the years 1999-2012 were collected, N = 11 065 330. We examined incentives present in part of the hospital funding system. First, we analyse trends in the proxy measures of diagnostic upcoding: can hospital behavioural changes be seen over time with regards to age composition, readmission rates, length of stay, comorbidity and mortality? Secondly, we examine specific patient groups to see if variations in the price incentive are related to probability of being coded as complicated. In the first years (1999-2003) there was an observed increase in the share of episodes coded as complicated, while the level has become more stable in the years 2004-2012. The analysis showed some indications of upcoding. However, we found no evidence of widespread upcoding fuelled by implicit price incentive, as other issues such as patient characteristics seem to be more important than the price differences. This study adds to previous research by testing individual level predictions. The added value of such analysis is to have better case mix control. We observe the presence of price effects even at individual level.
期刊介绍:
The focus of the International Journal of Health Economics and Management is on health care systems and on the behavior of consumers, patients, and providers of such services. The links among management, public policy, payment, and performance are core topics of the relaunched journal. The demand for health care and its cost remain central concerns. Even as medical innovation allows providers to improve the lives of their patients, questions remain about how to efficiently deliver health care services, how to pay for it, and who should pay for it. These are central questions facing innovators, providers, and payers in the public and private sectors. One key to answering these questions is to understand how people choose among alternative arrangements, either in markets or through the political process. The choices made by healthcare managers concerning the organization and production of that care are also crucial. There is an important connection between the management of a health care system and its economic performance. The primary audience for this journal will be health economists and researchers in health management, along with the larger group of health services researchers. In addition, research and policy analysis reported in the journal should be of interest to health care providers, managers and policymakers, who need to know about the pressures facing insurers and governments, with consequences for regulation and mandates. The editors of the journal encourage submissions that analyze the behavior and interaction of the actors in health care, viz. consumers, providers, insurers, and governments. Preference will be given to contributions that combine theoretical with empirical work, evaluate conflicting findings, present new information, or compare experiences between countries and jurisdictions. In addition to conventional research articles, the journal will include specific subsections for shorter concise research findings and cont ributions to management and policy that provide important descriptive data or arguments about what policies follow from research findings. The composition of the editorial board is designed to cover the range of interest among economics and management researchers.Officially cited as: Int J Health Econ ManagFrom 2001 to 2014 the journal was published as International Journal of Health Care Finance and Economics. (Articles published in Vol. 1-14 officially cited as: Int J Health Care Finance Econ)


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


