{"title":"肾内肾素-血管紧张素和糖尿病肾病替代途径的分子机制综述。","authors":"Elham Bahreini, Yousef Rezaei-Chianeh, Mohsen Nabi-Afjadi","doi":"10.1900/RDS.2021.17.1","DOIUrl":null,"url":null,"abstract":"<p><p>Uncontrolled or chronic hyperglycemia causes kidney failure induced by the dysfunction of biomolecules and upregulation of inflammatory cytokines and growth factors. The renin-angiotensin system (RAS) is incorporated in the regulation of renal hemodynamics. In a healthy state, local RAS is independent of systemic RAS. However, in pathological conditions such as chronic hyperglycemia, angiotensin II (Ang II) increases locally and causes tissue damage, mainly through the induction of oxidative stress, inflammation, and upregulation of some growth factors and their receptors. Such tissue events may cause disruption of the glomerular filtration barrier, thickening and hypertrophy of the glomerular basement membrane, microvascular hyperpermeability, proteinuria, and finally decrease in the glomerular filtration rate (GFR). Reduced GFR causes the kidney to sense falsely a low blood pressure condition and respond to it by stimulating systemic and local RAS. Therefore, patients with diabetic nephropathy (DN) suffer from chronic hypertension. In contrast to local RAS, there are alternative pathways in the kidney that act protectively by reducing tissue Ang II. Such autoregulatory and protective mechanisms are weakened in chronic kidney disease. Previously, it was presumed that systemic RAS inhibitors such as ACE inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) could prevent renal damage by controlling blood pressure and proteinuria. However, the progression of renal failure to end-stage renal disease (ESRD), despite such treatments, indicates the presence of factors other than Ang II. This review highlights the molecular mechanism in renal disease and discusses pharmaceutical and therapeutic approaches.</p>","PeriodicalId":34965,"journal":{"name":"Review of Diabetic Studies","volume":"17 1","pages":"1-10"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9380095/pdf/","citationCount":"11","resultStr":"{\"title\":\"Molecular Mechanisms Involved in Intrarenal Renin-Angiotensin and Alternative Pathways in Diabetic Nephropathy - A Review.\",\"authors\":\"Elham Bahreini, Yousef Rezaei-Chianeh, Mohsen Nabi-Afjadi\",\"doi\":\"10.1900/RDS.2021.17.1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Uncontrolled or chronic hyperglycemia causes kidney failure induced by the dysfunction of biomolecules and upregulation of inflammatory cytokines and growth factors. The renin-angiotensin system (RAS) is incorporated in the regulation of renal hemodynamics. In a healthy state, local RAS is independent of systemic RAS. However, in pathological conditions such as chronic hyperglycemia, angiotensin II (Ang II) increases locally and causes tissue damage, mainly through the induction of oxidative stress, inflammation, and upregulation of some growth factors and their receptors. Such tissue events may cause disruption of the glomerular filtration barrier, thickening and hypertrophy of the glomerular basement membrane, microvascular hyperpermeability, proteinuria, and finally decrease in the glomerular filtration rate (GFR). Reduced GFR causes the kidney to sense falsely a low blood pressure condition and respond to it by stimulating systemic and local RAS. Therefore, patients with diabetic nephropathy (DN) suffer from chronic hypertension. In contrast to local RAS, there are alternative pathways in the kidney that act protectively by reducing tissue Ang II. Such autoregulatory and protective mechanisms are weakened in chronic kidney disease. Previously, it was presumed that systemic RAS inhibitors such as ACE inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) could prevent renal damage by controlling blood pressure and proteinuria. However, the progression of renal failure to end-stage renal disease (ESRD), despite such treatments, indicates the presence of factors other than Ang II. This review highlights the molecular mechanism in renal disease and discusses pharmaceutical and therapeutic approaches.</p>\",\"PeriodicalId\":34965,\"journal\":{\"name\":\"Review of Diabetic Studies\",\"volume\":\"17 1\",\"pages\":\"1-10\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9380095/pdf/\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Review of Diabetic Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1900/RDS.2021.17.1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/5/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Review of Diabetic Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1900/RDS.2021.17.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/5/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Molecular Mechanisms Involved in Intrarenal Renin-Angiotensin and Alternative Pathways in Diabetic Nephropathy - A Review.
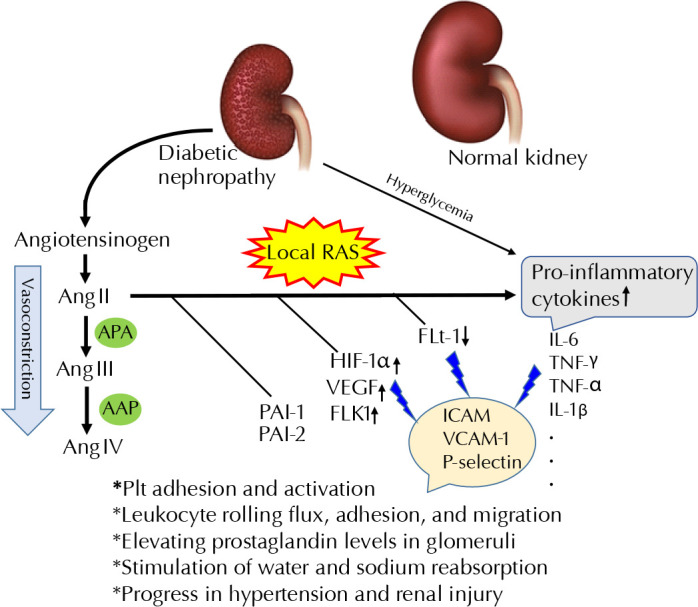
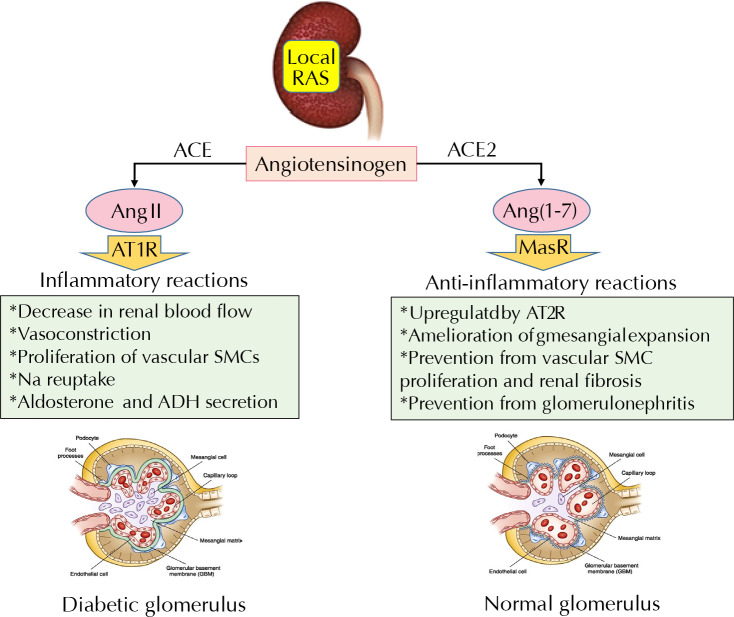
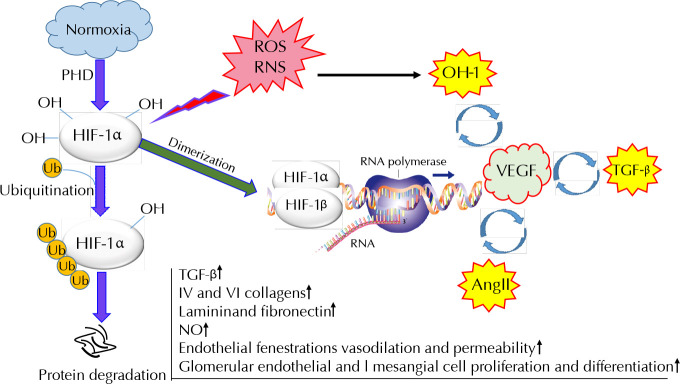
Uncontrolled or chronic hyperglycemia causes kidney failure induced by the dysfunction of biomolecules and upregulation of inflammatory cytokines and growth factors. The renin-angiotensin system (RAS) is incorporated in the regulation of renal hemodynamics. In a healthy state, local RAS is independent of systemic RAS. However, in pathological conditions such as chronic hyperglycemia, angiotensin II (Ang II) increases locally and causes tissue damage, mainly through the induction of oxidative stress, inflammation, and upregulation of some growth factors and their receptors. Such tissue events may cause disruption of the glomerular filtration barrier, thickening and hypertrophy of the glomerular basement membrane, microvascular hyperpermeability, proteinuria, and finally decrease in the glomerular filtration rate (GFR). Reduced GFR causes the kidney to sense falsely a low blood pressure condition and respond to it by stimulating systemic and local RAS. Therefore, patients with diabetic nephropathy (DN) suffer from chronic hypertension. In contrast to local RAS, there are alternative pathways in the kidney that act protectively by reducing tissue Ang II. Such autoregulatory and protective mechanisms are weakened in chronic kidney disease. Previously, it was presumed that systemic RAS inhibitors such as ACE inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) could prevent renal damage by controlling blood pressure and proteinuria. However, the progression of renal failure to end-stage renal disease (ESRD), despite such treatments, indicates the presence of factors other than Ang II. This review highlights the molecular mechanism in renal disease and discusses pharmaceutical and therapeutic approaches.
期刊介绍:
The Review of Diabetic Studies (RDS) is the society"s peer-reviewed journal published quarterly. The purpose of The RDS is to support and encourage research in biomedical diabetes-related science including areas such as endocrinology, immunology, epidemiology, genetics, cell-based research, developmental research, bioengineering and disease management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


