Jayshree South, Tina Gao, Andrew Collins, Arier Lee, Jason Turuwhenua, Joanna Black
{"title":"屈光参差和弱视的临床参差。","authors":"Jayshree South, Tina Gao, Andrew Collins, Arier Lee, Jason Turuwhenua, Joanna Black","doi":"10.22599/bioj.154","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Clinically, aniseikonia (a perceived difference in shape and image size between the eyes) is often neglected in anisometropic amblyopia due to assumed measurement difficulties. Therefore, we currently lack evidence on whether correction of aniseikonia is beneficial. This study aimed to determine whether subjective aniseikonia is measurable in anisometropia with or without amblyopia.</p><p><strong>Methods: </strong>Participants (15-52 years) with Anisometropic Amblyopia (n = 7), Anisometropia without amblyopia (n = 6) and Isometropic Controls (n = 6) were recruited. Subjective aniseikonia was measured using three clinical techniques: Robertson Technique (RT) (penlight and Maddox rod), Aniseikonia Inspector Version 3 (AI3), and the New Aniseikonia Test booklet (NAT), and a psychophysical adaptive method, the Contrast-balanced Aniseikonia Test (CAT), where dichoptic contrast adjustments compensate for any suppression.</p><p><strong>Results: </strong>Eighteen participants completed all tests, one Anisometropic Amblyopia participant could only complete the CAT and NAT due to fusion loss. The Anisometropic Amblyopia group exhibited the most aniseikonia (range -1.50-+10.50%) followed by Anisometropic Controls (range -3.30-+4.50%) and Isometropic Controls (range -1.50-+3.28%). There was a significant trend of more subjective aniseikonia with increasing amounts of anisometropia across all four tests (AI3 r = 0.630, p = 0.005; NAT r = 0.542, p = 0.017; RT r = 0.499, p = 0.035; CAT r = 0.440, p = 0.059. Bland Altman analysis demonstrated clinically significant levels of variability between the tests.</p><p><strong>Conclusions: </strong>Subjective aniseikonia can be reliably measured in patients with anisometropia and suppression. Subjective aniseikonia measurement is recommended as four of the most commonly used clinical tests did not support the 1% per dioptre rule of thumb.</p>","PeriodicalId":36083,"journal":{"name":"British and Irish Orthoptic Journal","volume":"16 1","pages":"44-54"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8269785/pdf/","citationCount":"5","resultStr":"{\"title\":\"Clinical Aniseikonia in Anisometropia and Amblyopia.\",\"authors\":\"Jayshree South, Tina Gao, Andrew Collins, Arier Lee, Jason Turuwhenua, Joanna Black\",\"doi\":\"10.22599/bioj.154\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Clinically, aniseikonia (a perceived difference in shape and image size between the eyes) is often neglected in anisometropic amblyopia due to assumed measurement difficulties. Therefore, we currently lack evidence on whether correction of aniseikonia is beneficial. This study aimed to determine whether subjective aniseikonia is measurable in anisometropia with or without amblyopia.</p><p><strong>Methods: </strong>Participants (15-52 years) with Anisometropic Amblyopia (n = 7), Anisometropia without amblyopia (n = 6) and Isometropic Controls (n = 6) were recruited. Subjective aniseikonia was measured using three clinical techniques: Robertson Technique (RT) (penlight and Maddox rod), Aniseikonia Inspector Version 3 (AI3), and the New Aniseikonia Test booklet (NAT), and a psychophysical adaptive method, the Contrast-balanced Aniseikonia Test (CAT), where dichoptic contrast adjustments compensate for any suppression.</p><p><strong>Results: </strong>Eighteen participants completed all tests, one Anisometropic Amblyopia participant could only complete the CAT and NAT due to fusion loss. The Anisometropic Amblyopia group exhibited the most aniseikonia (range -1.50-+10.50%) followed by Anisometropic Controls (range -3.30-+4.50%) and Isometropic Controls (range -1.50-+3.28%). There was a significant trend of more subjective aniseikonia with increasing amounts of anisometropia across all four tests (AI3 r = 0.630, p = 0.005; NAT r = 0.542, p = 0.017; RT r = 0.499, p = 0.035; CAT r = 0.440, p = 0.059. Bland Altman analysis demonstrated clinically significant levels of variability between the tests.</p><p><strong>Conclusions: </strong>Subjective aniseikonia can be reliably measured in patients with anisometropia and suppression. Subjective aniseikonia measurement is recommended as four of the most commonly used clinical tests did not support the 1% per dioptre rule of thumb.</p>\",\"PeriodicalId\":36083,\"journal\":{\"name\":\"British and Irish Orthoptic Journal\",\"volume\":\"16 1\",\"pages\":\"44-54\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-11-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8269785/pdf/\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"British and Irish Orthoptic Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22599/bioj.154\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"British and Irish Orthoptic Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22599/bioj.154","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 5
摘要
目的:临床上,由于假定的测量困难,在屈光参差性弱视中,往往忽略了斜视(眼睛之间形状和图像大小的感知差异)。因此,我们目前缺乏证据证明矫正斜视是否有益。本研究旨在确定主观性参差是否可在参差伴弱视或不伴弱视中测量。方法:招募参差性弱视(n = 7)、无弱视参差性弱视(n = 6)和参差性对照(n = 6)的参与者(15-52岁)。主观差异使用三种临床技术进行测量:罗伯逊技术(RT) (penlight和Maddox棒),差异检查版本3 (AI3)和新差异测试手册(NAT),以及一种心理物理适应性方法,对比平衡差异测试(CAT),其中二元对比调整补偿任何抑制。结果:18名参与者完成了所有测试,1名参差弱视参与者因融合缺失只能完成CAT和NAT测试。屈光参差组屈光参差程度最高(-1.50 ~ +10.50%),屈光参差对照组次之(-3.30 ~ +4.50%),屈光参差对照组次之(-1.50 ~ +3.28%)。在所有四项测试中,随着参差程度的增加,主观参差程度的增加有明显的趋势(AI3 r = 0.630, p = 0.005;NAT r = 0.542, p = 0.017;RT = 0.499, p = 0.035;CAT r = 0.440, p = 0.059。Bland Altman分析显示两种测试之间存在显著的临床差异。结论:在屈光参差和屈光抑制患者中,主观参差可可靠测量。主观斜视测量是推荐的,因为四种最常用的临床试验不支持每屈光度1%的经验法则。
Clinical Aniseikonia in Anisometropia and Amblyopia.
Purpose: Clinically, aniseikonia (a perceived difference in shape and image size between the eyes) is often neglected in anisometropic amblyopia due to assumed measurement difficulties. Therefore, we currently lack evidence on whether correction of aniseikonia is beneficial. This study aimed to determine whether subjective aniseikonia is measurable in anisometropia with or without amblyopia.
Methods: Participants (15-52 years) with Anisometropic Amblyopia (n = 7), Anisometropia without amblyopia (n = 6) and Isometropic Controls (n = 6) were recruited. Subjective aniseikonia was measured using three clinical techniques: Robertson Technique (RT) (penlight and Maddox rod), Aniseikonia Inspector Version 3 (AI3), and the New Aniseikonia Test booklet (NAT), and a psychophysical adaptive method, the Contrast-balanced Aniseikonia Test (CAT), where dichoptic contrast adjustments compensate for any suppression.
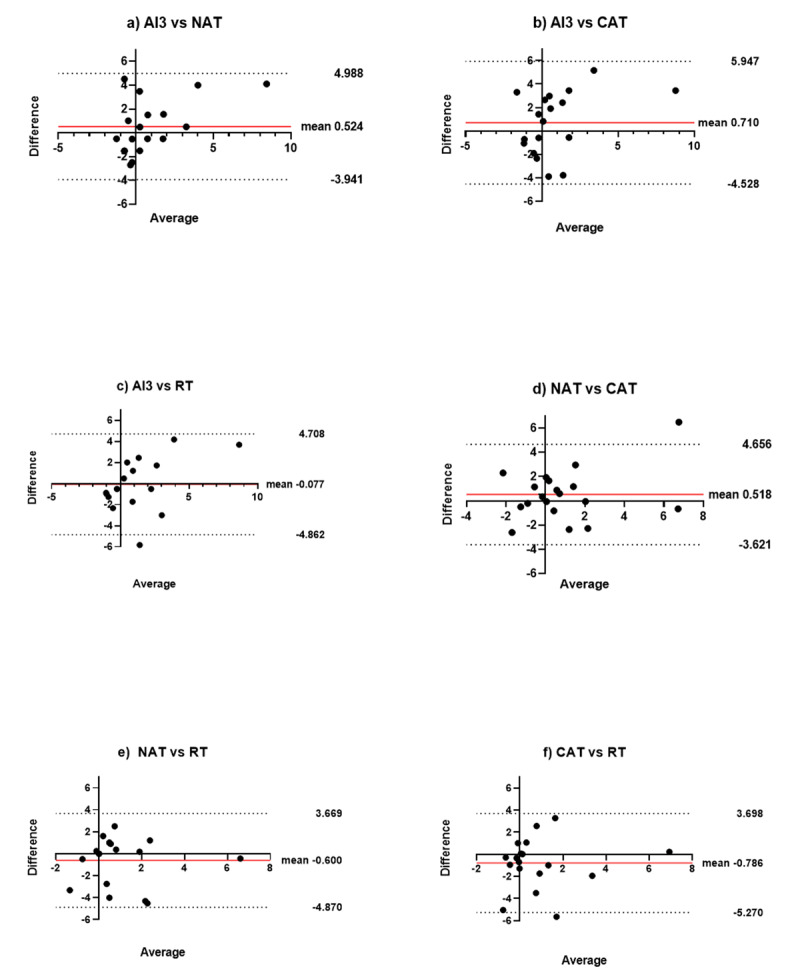
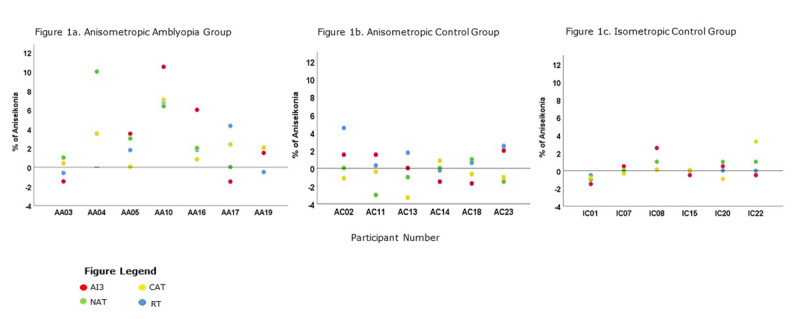
Results: Eighteen participants completed all tests, one Anisometropic Amblyopia participant could only complete the CAT and NAT due to fusion loss. The Anisometropic Amblyopia group exhibited the most aniseikonia (range -1.50-+10.50%) followed by Anisometropic Controls (range -3.30-+4.50%) and Isometropic Controls (range -1.50-+3.28%). There was a significant trend of more subjective aniseikonia with increasing amounts of anisometropia across all four tests (AI3 r = 0.630, p = 0.005; NAT r = 0.542, p = 0.017; RT r = 0.499, p = 0.035; CAT r = 0.440, p = 0.059. Bland Altman analysis demonstrated clinically significant levels of variability between the tests.
Conclusions: Subjective aniseikonia can be reliably measured in patients with anisometropia and suppression. Subjective aniseikonia measurement is recommended as four of the most commonly used clinical tests did not support the 1% per dioptre rule of thumb.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


