F Flottmann, N van Horn, M E Maros, R McDonough, M Deb-Chatterji, A Alegiani, G Thomalla, U Hanning, J Fiehler, C Brekenfeld
{"title":"早期TICI 2b或晚期TICI 3-完美是好的敌人吗?","authors":"F Flottmann, N van Horn, M E Maros, R McDonough, M Deb-Chatterji, A Alegiani, G Thomalla, U Hanning, J Fiehler, C Brekenfeld","doi":"10.1007/s00062-021-01048-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>A Thrombolysis in Cerebral Infarction (TICI) score of 3 has been established as therapeutic goal in endovascular therapy (EVT) for acute ischemic stroke; however, in the case of early TICI2b reperfusion, the question remains whether to stop the procedure or to continue in the pursuit of perfection (i.e., TICI 2c/3).</p><p><strong>Methods: </strong>A total of 6635 patients were screened from the German Stroke Registry. Patients who underwent EVT for occlusion of the middle cerebral artery (M1 segment), with final TICI score of 2b/3 were included. Multivariable logistic regression was performed with functional independence (modified Rankin Scale, mRS at day 90 of 0-2) as the dependent variable.</p><p><strong>Results: </strong>Of 1497 patients, 586 (39.1%) met inclusion criteria with a final TICI score of 2b and 911 (60.9%) with a TICI score of 3. Patients who achieved first-pass TICI3 showed highest odds of functional independence (Odds ratio [OR] 1.71, 95% confidence interval [95% CI] 1.18-2.47). Patients who achieved TICI2b with the second pass (OR 0.53, 95% CI 0.31-0.89) or with three or more passes (OR 0.44, 95% CI 0.27-0.70) had significantly worse clinical outcomes compared to first-pass TICI2b. TICI3 at the second pass was by trend better than first-pass TICI2b (OR 1.55, 95% CI 0.98-2.45), but TICI3 after 3 or more passes (OR 0.93, 95% CI 0.57-1.50) was not significantly different from first-pass TICI2b.</p><p><strong>Conclusion: </strong>First-pass TICI2b was superior to TICI2b after ≥ 2 retrievals and comparable to TICI3 at ≥ 3 retrievals. The potential benefit in outcome after achieving TICI3 following further retrieval attempts after first-pass TICI2b need to be weighed against the risks.</p>","PeriodicalId":49298,"journal":{"name":"Clinical Neuroradiology","volume":"32 2","pages":"353-360"},"PeriodicalIF":2.4000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s00062-021-01048-8","citationCount":"11","resultStr":"{\"title\":\"Early TICI 2b or Late TICI 3-Is Perfect the Enemy of Good?\",\"authors\":\"F Flottmann, N van Horn, M E Maros, R McDonough, M Deb-Chatterji, A Alegiani, G Thomalla, U Hanning, J Fiehler, C Brekenfeld\",\"doi\":\"10.1007/s00062-021-01048-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>A Thrombolysis in Cerebral Infarction (TICI) score of 3 has been established as therapeutic goal in endovascular therapy (EVT) for acute ischemic stroke; however, in the case of early TICI2b reperfusion, the question remains whether to stop the procedure or to continue in the pursuit of perfection (i.e., TICI 2c/3).</p><p><strong>Methods: </strong>A total of 6635 patients were screened from the German Stroke Registry. Patients who underwent EVT for occlusion of the middle cerebral artery (M1 segment), with final TICI score of 2b/3 were included. Multivariable logistic regression was performed with functional independence (modified Rankin Scale, mRS at day 90 of 0-2) as the dependent variable.</p><p><strong>Results: </strong>Of 1497 patients, 586 (39.1%) met inclusion criteria with a final TICI score of 2b and 911 (60.9%) with a TICI score of 3. Patients who achieved first-pass TICI3 showed highest odds of functional independence (Odds ratio [OR] 1.71, 95% confidence interval [95% CI] 1.18-2.47). Patients who achieved TICI2b with the second pass (OR 0.53, 95% CI 0.31-0.89) or with three or more passes (OR 0.44, 95% CI 0.27-0.70) had significantly worse clinical outcomes compared to first-pass TICI2b. TICI3 at the second pass was by trend better than first-pass TICI2b (OR 1.55, 95% CI 0.98-2.45), but TICI3 after 3 or more passes (OR 0.93, 95% CI 0.57-1.50) was not significantly different from first-pass TICI2b.</p><p><strong>Conclusion: </strong>First-pass TICI2b was superior to TICI2b after ≥ 2 retrievals and comparable to TICI3 at ≥ 3 retrievals. The potential benefit in outcome after achieving TICI3 following further retrieval attempts after first-pass TICI2b need to be weighed against the risks.</p>\",\"PeriodicalId\":49298,\"journal\":{\"name\":\"Clinical Neuroradiology\",\"volume\":\"32 2\",\"pages\":\"353-360\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2022-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1007/s00062-021-01048-8\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Neuroradiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00062-021-01048-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Neuroradiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00062-021-01048-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/6/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 11
摘要
背景与目的:脑梗死溶栓(TICI)评分为3分已被确立为急性缺血性卒中血管内治疗(EVT)的治疗目标;然而,在早期TICI2b再灌注的情况下,问题仍然是停止该程序还是继续追求完美(即tici2c /3)。方法:从德国卒中登记中心共筛选6635例患者。纳入因大脑中动脉(M1段)闭塞而行EVT的患者,最终TICI评分为2b/3。以功能独立性(修正Rankin量表,0-2的第90天mRS)为因变量进行多变量logistic回归。结果:1497例患者中,586例(39.1%)符合纳入标准,最终TICI评分为2b, 911例(60.9%)TICI评分为3。达到首次通过的患者功能独立的几率最高(优势比[OR] 1.71, 95%可信区间[95% CI] 1.18-2.47)。第二次通过(OR 0.53, 95% CI 0.31-0.89)或三次或三次以上通过(OR 0.44, 95% CI 0.27-0.70)的患者与第一次通过的患者相比,临床结果明显更差。从趋势上看,第二次通过的TICI3优于第一次通过的TICI2b (OR 1.55, 95% CI 0.98-2.45),但3次或更多次通过后的TICI3 (OR 0.93, 95% CI 0.57-1.50)与第一次通过的TICI2b无显著差异。结论:第一次通过的TICI2b在≥ 2次检索后优于TICI2b,在≥ 3次检索时与TICI3相当。在第一次通过TICI2b后,在进一步检索尝试后达到TICI3的潜在收益需要与风险进行权衡。
Early TICI 2b or Late TICI 3-Is Perfect the Enemy of Good?
Background and purpose: A Thrombolysis in Cerebral Infarction (TICI) score of 3 has been established as therapeutic goal in endovascular therapy (EVT) for acute ischemic stroke; however, in the case of early TICI2b reperfusion, the question remains whether to stop the procedure or to continue in the pursuit of perfection (i.e., TICI 2c/3).
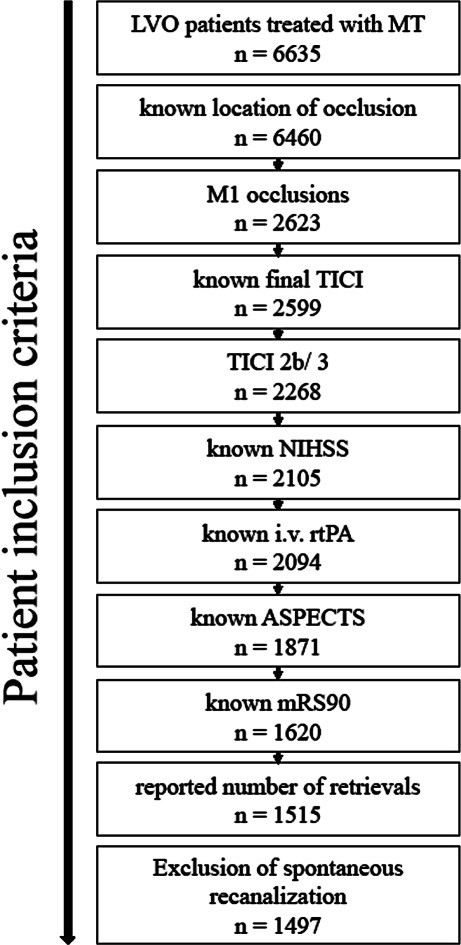
Methods: A total of 6635 patients were screened from the German Stroke Registry. Patients who underwent EVT for occlusion of the middle cerebral artery (M1 segment), with final TICI score of 2b/3 were included. Multivariable logistic regression was performed with functional independence (modified Rankin Scale, mRS at day 90 of 0-2) as the dependent variable.
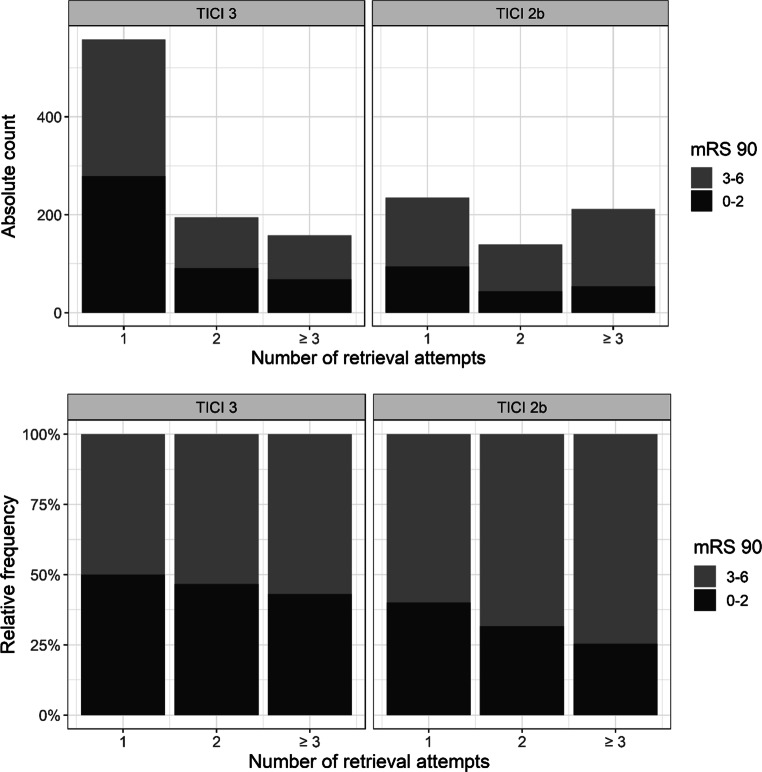
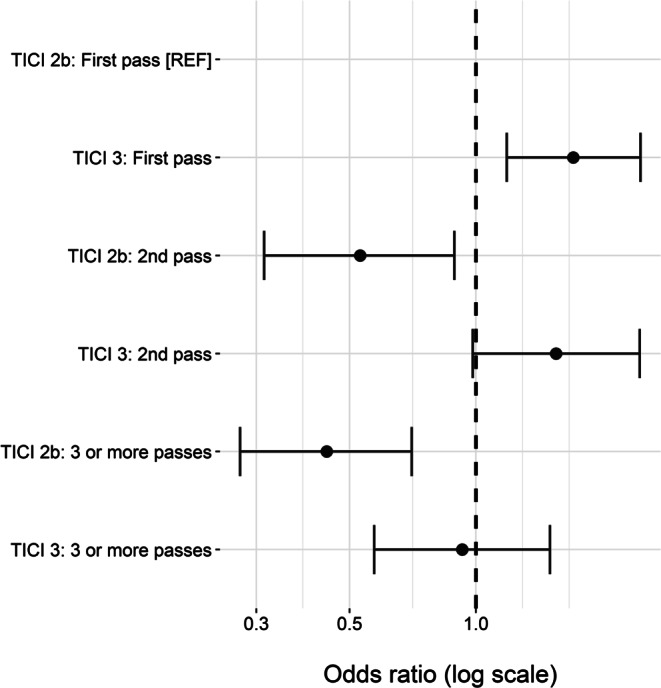
Results: Of 1497 patients, 586 (39.1%) met inclusion criteria with a final TICI score of 2b and 911 (60.9%) with a TICI score of 3. Patients who achieved first-pass TICI3 showed highest odds of functional independence (Odds ratio [OR] 1.71, 95% confidence interval [95% CI] 1.18-2.47). Patients who achieved TICI2b with the second pass (OR 0.53, 95% CI 0.31-0.89) or with three or more passes (OR 0.44, 95% CI 0.27-0.70) had significantly worse clinical outcomes compared to first-pass TICI2b. TICI3 at the second pass was by trend better than first-pass TICI2b (OR 1.55, 95% CI 0.98-2.45), but TICI3 after 3 or more passes (OR 0.93, 95% CI 0.57-1.50) was not significantly different from first-pass TICI2b.
Conclusion: First-pass TICI2b was superior to TICI2b after ≥ 2 retrievals and comparable to TICI3 at ≥ 3 retrievals. The potential benefit in outcome after achieving TICI3 following further retrieval attempts after first-pass TICI2b need to be weighed against the risks.
期刊介绍:
Clinical Neuroradiology provides current information, original contributions, and reviews in the field of neuroradiology. An interdisciplinary approach is accomplished by diagnostic and therapeutic contributions related to associated subjects.
The international coverage and relevance of the journal is underlined by its being the official journal of the German, Swiss, and Austrian Societies of Neuroradiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


