{"title":"清醒纤维插管的麻醉:超声引导的气道神经阻滞与利多卡因超声雾化。","authors":"Jharana Mohanta, Ajit Kumar, Ashutosh Kaushal, Praveen Talawar, Priyanka Gupta, Gaurav Jain","doi":"10.15190/d.2021.4","DOIUrl":null,"url":null,"abstract":"Background: In anticipated difficult airway, awake fiberoptic guided intubation should be the ideal plan of management. It requires sufficient upper airway anesthesia for patient’s comfort and cooperation. We compared the efficacy of ultrasound guided airway nerve blocks and ultrasonic nebulisation with lignocaine for airway anesthesia before performing awake fibreoptic guided intubation. Methods: This prospective, randomised study included sixty consenting adult patients of both genders (American Society of Anesthesiologists' physical status 1–3) with anticipated difficult airway undergoing surgery. Ultrasound guided airway nerve blocks group received ultrasound-guided bilateral superior laryngeal (1 ml of 2% lignocaine) and transtracheal recurrent laryngeal (2 ml of 2% lignocaine) airway nerve blocks and ultrasonic nebulisation with lignocaine group received ultrasonic nebulisation of 4 ml of lignocaine 4%. The primary outcome was to compare the time required to intubate, whereas the secondary outcomes were to compare cough reflex and gag reflex, hemodynamic changes, number of attempts required, and comfort score during awake fibreoptic guided intubation in both the groups. Results: The time taken for intubation was significantly lower in the ultrasound guided airway nerve blocks group 69.27±21.85 s than ultrasonic nebulisation with lignocaine group 92.43 ± 42.90 s (p = 0.015). Hemodynamic variables changed during the procedure but the values were comparable in both groups. There were no statistical differences in cough and gag reflexes, number of attempts, and comfort score in both groups. Conclusions: This study shows that significant lesser time required for performing awake fiberoptic intubation when patient received ultrasound guided airway nerve block in comparison to ultrasonic nebulisation for airway anaesthesia.","PeriodicalId":72829,"journal":{"name":"Discoveries (Craiova, Romania)","volume":"9 1","pages":"e125"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8140785/pdf/","citationCount":"8","resultStr":"{\"title\":\"Anaesthesia for Awake Fiberoptic Intubation: Ultrasound-Guided Airway Nerve Block versus Ultrasonic Nebulisation with Lignocaine.\",\"authors\":\"Jharana Mohanta, Ajit Kumar, Ashutosh Kaushal, Praveen Talawar, Priyanka Gupta, Gaurav Jain\",\"doi\":\"10.15190/d.2021.4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Background: In anticipated difficult airway, awake fiberoptic guided intubation should be the ideal plan of management. It requires sufficient upper airway anesthesia for patient’s comfort and cooperation. We compared the efficacy of ultrasound guided airway nerve blocks and ultrasonic nebulisation with lignocaine for airway anesthesia before performing awake fibreoptic guided intubation. Methods: This prospective, randomised study included sixty consenting adult patients of both genders (American Society of Anesthesiologists' physical status 1–3) with anticipated difficult airway undergoing surgery. Ultrasound guided airway nerve blocks group received ultrasound-guided bilateral superior laryngeal (1 ml of 2% lignocaine) and transtracheal recurrent laryngeal (2 ml of 2% lignocaine) airway nerve blocks and ultrasonic nebulisation with lignocaine group received ultrasonic nebulisation of 4 ml of lignocaine 4%. The primary outcome was to compare the time required to intubate, whereas the secondary outcomes were to compare cough reflex and gag reflex, hemodynamic changes, number of attempts required, and comfort score during awake fibreoptic guided intubation in both the groups. Results: The time taken for intubation was significantly lower in the ultrasound guided airway nerve blocks group 69.27±21.85 s than ultrasonic nebulisation with lignocaine group 92.43 ± 42.90 s (p = 0.015). Hemodynamic variables changed during the procedure but the values were comparable in both groups. There were no statistical differences in cough and gag reflexes, number of attempts, and comfort score in both groups. Conclusions: This study shows that significant lesser time required for performing awake fiberoptic intubation when patient received ultrasound guided airway nerve block in comparison to ultrasonic nebulisation for airway anaesthesia.\",\"PeriodicalId\":72829,\"journal\":{\"name\":\"Discoveries (Craiova, Romania)\",\"volume\":\"9 1\",\"pages\":\"e125\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-03-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8140785/pdf/\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Discoveries (Craiova, Romania)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15190/d.2021.4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Discoveries (Craiova, Romania)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15190/d.2021.4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Anaesthesia for Awake Fiberoptic Intubation: Ultrasound-Guided Airway Nerve Block versus Ultrasonic Nebulisation with Lignocaine.
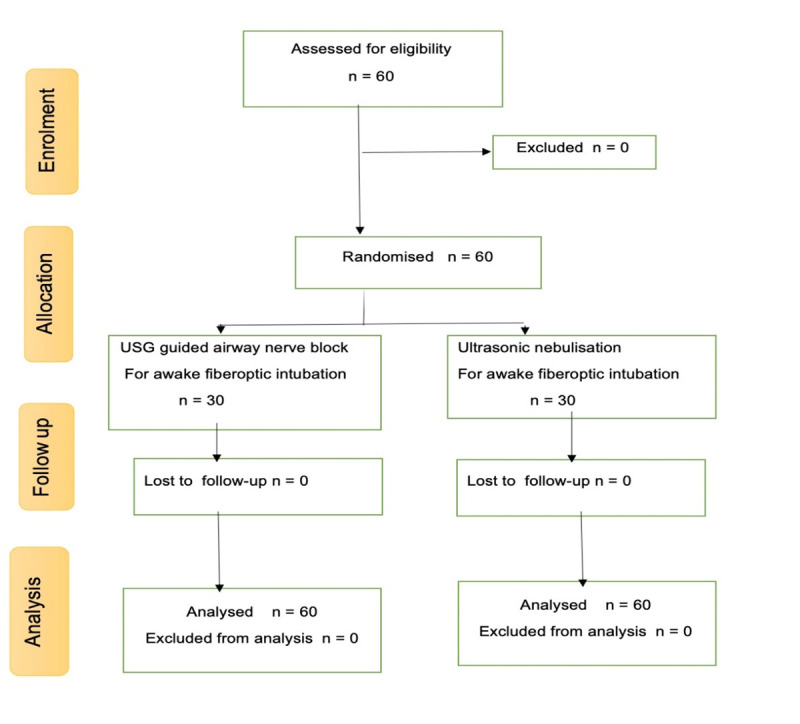
Background: In anticipated difficult airway, awake fiberoptic guided intubation should be the ideal plan of management. It requires sufficient upper airway anesthesia for patient’s comfort and cooperation. We compared the efficacy of ultrasound guided airway nerve blocks and ultrasonic nebulisation with lignocaine for airway anesthesia before performing awake fibreoptic guided intubation. Methods: This prospective, randomised study included sixty consenting adult patients of both genders (American Society of Anesthesiologists' physical status 1–3) with anticipated difficult airway undergoing surgery. Ultrasound guided airway nerve blocks group received ultrasound-guided bilateral superior laryngeal (1 ml of 2% lignocaine) and transtracheal recurrent laryngeal (2 ml of 2% lignocaine) airway nerve blocks and ultrasonic nebulisation with lignocaine group received ultrasonic nebulisation of 4 ml of lignocaine 4%. The primary outcome was to compare the time required to intubate, whereas the secondary outcomes were to compare cough reflex and gag reflex, hemodynamic changes, number of attempts required, and comfort score during awake fibreoptic guided intubation in both the groups. Results: The time taken for intubation was significantly lower in the ultrasound guided airway nerve blocks group 69.27±21.85 s than ultrasonic nebulisation with lignocaine group 92.43 ± 42.90 s (p = 0.015). Hemodynamic variables changed during the procedure but the values were comparable in both groups. There were no statistical differences in cough and gag reflexes, number of attempts, and comfort score in both groups. Conclusions: This study shows that significant lesser time required for performing awake fiberoptic intubation when patient received ultrasound guided airway nerve block in comparison to ultrasonic nebulisation for airway anaesthesia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


