{"title":"吲哚菁绿荧光成像在胆囊、肝切除术胆道造影中的应用效果。","authors":"Hideki Shibata, Takeshi Aoki, Tomotake Koizumi, Tomokazu Kusano, Tatsuya Yamazaki, Kazuhiko Saito, Takahito Hirai, Kodai Tomioka, Yusuke Wada, Tomoki Hakozaki, Yoshihiko Tashiro, Koji Nogaki, Kosuke Yamada, Kazuhiro Matsuda, Akira Fujimori, Yuta Enami, Masahiko Murakami","doi":"10.2147/CEG.S275985","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Bile duct injury is one of the most serious complications of laparoscopic cholecystectomy. Intraoperative indocyanine green (ICG) cholangiography is a safe and useful navigation modality for confirming the biliary anatomy. ICG cholangiography is expected to be a routine method for helping avoid bile duct injuries.</p><p><strong>Patients and methods: </strong>We examined 25 patients who underwent intraoperative cholangiography using ICG fluorescence. Two methods of ICG injection are used: intrabiliary injection (percutaneous transhepatic gallbladder drainage [PTGBD], gallbladder [GB] puncture and endoscopic nasobiliary drainage [ENBD]) at a dosage of 0.025 mg during the operation or intravenous injection with 2.5 mg ICG preoperatively.</p><p><strong>Results: </strong>There were 24 patients who underwent laparoscopic cholecystectomy and 1 patient who underwent hepatectomy. For laparoscopic cholecystectomy, the average operation time was 127 (50-197) minutes, and estimated blood loss was 43.2 (0-400) g. The ICG administration route was intravenous injections in 12 cases and intrabiliary injection in 12 cases (GB injection: 3 cases, PTGBD: 8 cases, ENBD:1 case). The course of the biliary tree was able to be confirmed in all cases that received direct injection into the biliary tract, whereas bile structures were recognizable in only 10 cases (83.3%) with intravenous injection. The postoperative hospital stay was 4.6 (3-9) days, and no postoperative complications (Clavien-Dindo ≧IIIa) were observed. For hepatectomy, a tumor located near the left Glissonian pedicle was resected using a fluorescence image guide. Biliary structures were fluorescent without injury after resecting the tumor. No adverse events due to ICG administration were observed, and the procedure was able to be performed safely.</p><p><strong>Conclusion: </strong>ICG fluorescence imaging allows surgeons to visualize the course of the biliary tree in real time during cholecystectomy and hepatectomy. This is considered essential for hepatobiliary surgery to prevent biliary tree injury and ensure safe surgery.</p>","PeriodicalId":10208,"journal":{"name":"Clinical and Experimental Gastroenterology","volume":"14 ","pages":"145-154"},"PeriodicalIF":2.5000,"publicationDate":"2021-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/c8/ceg-14-145.PMC8096340.pdf","citationCount":"8","resultStr":"{\"title\":\"The Efficacy of Intraoperative Fluorescent Imaging Using Indocyanine Green for Cholangiography During Cholecystectomy and Hepatectomy.\",\"authors\":\"Hideki Shibata, Takeshi Aoki, Tomotake Koizumi, Tomokazu Kusano, Tatsuya Yamazaki, Kazuhiko Saito, Takahito Hirai, Kodai Tomioka, Yusuke Wada, Tomoki Hakozaki, Yoshihiko Tashiro, Koji Nogaki, Kosuke Yamada, Kazuhiro Matsuda, Akira Fujimori, Yuta Enami, Masahiko Murakami\",\"doi\":\"10.2147/CEG.S275985\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Bile duct injury is one of the most serious complications of laparoscopic cholecystectomy. Intraoperative indocyanine green (ICG) cholangiography is a safe and useful navigation modality for confirming the biliary anatomy. ICG cholangiography is expected to be a routine method for helping avoid bile duct injuries.</p><p><strong>Patients and methods: </strong>We examined 25 patients who underwent intraoperative cholangiography using ICG fluorescence. Two methods of ICG injection are used: intrabiliary injection (percutaneous transhepatic gallbladder drainage [PTGBD], gallbladder [GB] puncture and endoscopic nasobiliary drainage [ENBD]) at a dosage of 0.025 mg during the operation or intravenous injection with 2.5 mg ICG preoperatively.</p><p><strong>Results: </strong>There were 24 patients who underwent laparoscopic cholecystectomy and 1 patient who underwent hepatectomy. For laparoscopic cholecystectomy, the average operation time was 127 (50-197) minutes, and estimated blood loss was 43.2 (0-400) g. The ICG administration route was intravenous injections in 12 cases and intrabiliary injection in 12 cases (GB injection: 3 cases, PTGBD: 8 cases, ENBD:1 case). The course of the biliary tree was able to be confirmed in all cases that received direct injection into the biliary tract, whereas bile structures were recognizable in only 10 cases (83.3%) with intravenous injection. The postoperative hospital stay was 4.6 (3-9) days, and no postoperative complications (Clavien-Dindo ≧IIIa) were observed. For hepatectomy, a tumor located near the left Glissonian pedicle was resected using a fluorescence image guide. Biliary structures were fluorescent without injury after resecting the tumor. No adverse events due to ICG administration were observed, and the procedure was able to be performed safely.</p><p><strong>Conclusion: </strong>ICG fluorescence imaging allows surgeons to visualize the course of the biliary tree in real time during cholecystectomy and hepatectomy. This is considered essential for hepatobiliary surgery to prevent biliary tree injury and ensure safe surgery.</p>\",\"PeriodicalId\":10208,\"journal\":{\"name\":\"Clinical and Experimental Gastroenterology\",\"volume\":\"14 \",\"pages\":\"145-154\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2021-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/c8/ceg-14-145.PMC8096340.pdf\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEG.S275985\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEG.S275985","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
The Efficacy of Intraoperative Fluorescent Imaging Using Indocyanine Green for Cholangiography During Cholecystectomy and Hepatectomy.
Purpose: Bile duct injury is one of the most serious complications of laparoscopic cholecystectomy. Intraoperative indocyanine green (ICG) cholangiography is a safe and useful navigation modality for confirming the biliary anatomy. ICG cholangiography is expected to be a routine method for helping avoid bile duct injuries.
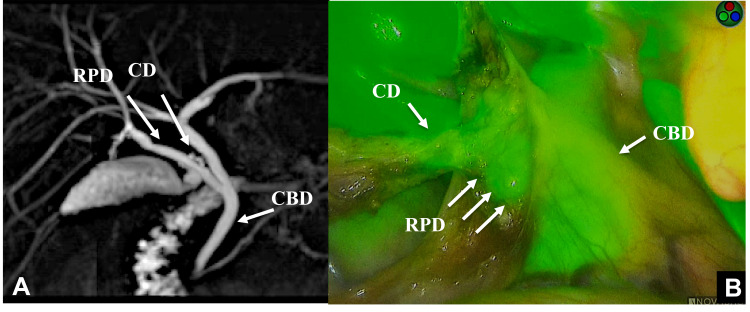
Patients and methods: We examined 25 patients who underwent intraoperative cholangiography using ICG fluorescence. Two methods of ICG injection are used: intrabiliary injection (percutaneous transhepatic gallbladder drainage [PTGBD], gallbladder [GB] puncture and endoscopic nasobiliary drainage [ENBD]) at a dosage of 0.025 mg during the operation or intravenous injection with 2.5 mg ICG preoperatively.
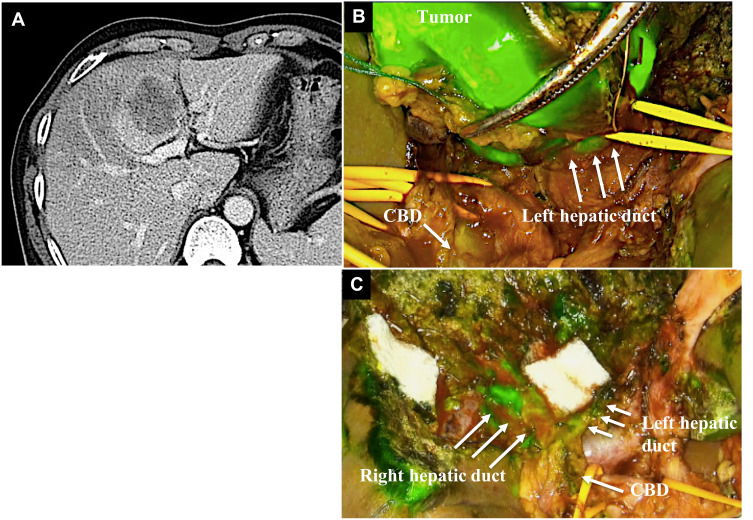
Results: There were 24 patients who underwent laparoscopic cholecystectomy and 1 patient who underwent hepatectomy. For laparoscopic cholecystectomy, the average operation time was 127 (50-197) minutes, and estimated blood loss was 43.2 (0-400) g. The ICG administration route was intravenous injections in 12 cases and intrabiliary injection in 12 cases (GB injection: 3 cases, PTGBD: 8 cases, ENBD:1 case). The course of the biliary tree was able to be confirmed in all cases that received direct injection into the biliary tract, whereas bile structures were recognizable in only 10 cases (83.3%) with intravenous injection. The postoperative hospital stay was 4.6 (3-9) days, and no postoperative complications (Clavien-Dindo ≧IIIa) were observed. For hepatectomy, a tumor located near the left Glissonian pedicle was resected using a fluorescence image guide. Biliary structures were fluorescent without injury after resecting the tumor. No adverse events due to ICG administration were observed, and the procedure was able to be performed safely.
Conclusion: ICG fluorescence imaging allows surgeons to visualize the course of the biliary tree in real time during cholecystectomy and hepatectomy. This is considered essential for hepatobiliary surgery to prevent biliary tree injury and ensure safe surgery.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


