{"title":"在塞内加尔一个分散的城市艾滋病诊所接受至少 12 个月一线抗逆转录病毒疗法的成年患者中,HIV-1 病毒学失败和耐药性较高。","authors":"Aristid Ekollo Mbange, Abou Abdallah Malick Diouara, Halimatou Diop-Ndiaye, Ndèye Aminata Diaw Diouf, Ndèye Fatou Ngom-Ngueye, Kine Ndiaye Touré, Ahmed Dieng, Seynabou Lô, Mamadou Fall, Wilfred Fon Mbacham, Souleymane Mboup, Coumba Touré-Kane","doi":"10.1177/11786337211014503","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The feasibility of antiretroviral therapy (ART) monitoring remains problematic in decentralized HIV clinic settings of sub-Saharan Africa. We assessed the rates and correlates of HIV-1 virological failure (VF) and drug resistance (DR) in 2 pre-test-and-treat urban clinic settings of Senegal.</p><p><strong>Methods: </strong>Consenting HIV-1-infected adults (⩾18 years) receiving first-line ART for ⩾12 months were cross-sectionally enrolled between January and March 2015, at the referral outpatient treatment center of Dakar (n = 151) and decentralized regional hospital of Saint-Louis (n = 127). In the 12 months preceding plasma specimens' collection patients at Saint-Louis had no viral load (VL) testing. Significant predictors of VF (VL ⩾ 1000 copies/ml) and DR (clinically relevant mutations) were determined using binomial logistic regression in R software.</p><p><strong>Results: </strong>Of the 278 adults on EFV-/NVP-based regimens, 32 (11.5% [95%CI: 8.0-15.9]) experienced VF. Failing and non-failing patients had comparable median time [interquartile] on ART (69.5 [23.0-89.5] vs 64.0 [34.0-99.0] months; <i>P</i> = .46, Mann-Whitney <i>U</i>-test). Of the 27 viraemic isolates successfully genotyped, 20 (74.1%) carried DR mutations; most frequent were M184VI (55.6%), K103N (37.1%), thymidine analog mutations (29.6%), Y181CY (22.2%). The pattern of mutations did not always correspond to the ongoing treatment. The adjusted odds of VF was significantly associated with the decentralized clinic site (<i>P</i> < .001) and CD4 < 350 cells/mm<sup>3</sup> (<i>P</i> < .006). Strong correlates of DR also included Saint-Louis (<i>P</i> < .009), CD4 < 350 cells/mm<sup>3</sup> (<i>P</i> <. 001), and nevirapine-based therapies (comparator: efavirenz-based therapies; <i>P</i> < .027). In stratification analyses by site, higher rate of VF at Saint-Louis (20.5% [95%CI: 13.8-28.5] vs 4.0% [95%CI: 1.5-8.5] in Dakar) was associated with nevirapine-based therapies (OR = 3.34 [1.07-11.75], <i>P</i> = .038), self-reported missing doses (OR = 3.30 [1.13-10.24], <i>P</i> = .029), and medical appointments (OR = 2.91 [1.05-8.47], <i>P</i> = .039) in the last 1 and 12 months(s), respectively. The higher rate of DR at Saint-Louis (12.9% [95%CI: 7.6-20.1] vs 2.7% [95%CI: 0.7-6.7] in Dakar) was associated with nevirapine-based therapies (OR = 5.13 [1.12-37.35], <i>P</i> = .035).</p><p><strong>Conclusion: </strong>At decentralized urban settings, there is need for enhanced virological monitoring and adherence support. HIV programs in Senegal should intensify early HIV diagnosis for effective test-and-treat. These interventions, in addition to the superiority of efavirenz-based therapies provide a favorable framework for transitioning to the recommended potent drug dolutegravir, thereby ensuring its long-term use.</p>","PeriodicalId":13671,"journal":{"name":"Infectious Diseases","volume":"14 ","pages":"11786337211014503"},"PeriodicalIF":2.3000,"publicationDate":"2021-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/aa/d3/10.1177_11786337211014503.PMC8120520.pdf","citationCount":"0","resultStr":"{\"title\":\"High HIV-1 Virological Failure and Drug Resistance among Adult Patients Receiving First-Line ART for At least 12 Months at a Decentralized Urban HIV Clinic Setting in Senegal before the Test-and-Treat.\",\"authors\":\"Aristid Ekollo Mbange, Abou Abdallah Malick Diouara, Halimatou Diop-Ndiaye, Ndèye Aminata Diaw Diouf, Ndèye Fatou Ngom-Ngueye, Kine Ndiaye Touré, Ahmed Dieng, Seynabou Lô, Mamadou Fall, Wilfred Fon Mbacham, Souleymane Mboup, Coumba Touré-Kane\",\"doi\":\"10.1177/11786337211014503\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The feasibility of antiretroviral therapy (ART) monitoring remains problematic in decentralized HIV clinic settings of sub-Saharan Africa. We assessed the rates and correlates of HIV-1 virological failure (VF) and drug resistance (DR) in 2 pre-test-and-treat urban clinic settings of Senegal.</p><p><strong>Methods: </strong>Consenting HIV-1-infected adults (⩾18 years) receiving first-line ART for ⩾12 months were cross-sectionally enrolled between January and March 2015, at the referral outpatient treatment center of Dakar (n = 151) and decentralized regional hospital of Saint-Louis (n = 127). In the 12 months preceding plasma specimens' collection patients at Saint-Louis had no viral load (VL) testing. Significant predictors of VF (VL ⩾ 1000 copies/ml) and DR (clinically relevant mutations) were determined using binomial logistic regression in R software.</p><p><strong>Results: </strong>Of the 278 adults on EFV-/NVP-based regimens, 32 (11.5% [95%CI: 8.0-15.9]) experienced VF. Failing and non-failing patients had comparable median time [interquartile] on ART (69.5 [23.0-89.5] vs 64.0 [34.0-99.0] months; <i>P</i> = .46, Mann-Whitney <i>U</i>-test). Of the 27 viraemic isolates successfully genotyped, 20 (74.1%) carried DR mutations; most frequent were M184VI (55.6%), K103N (37.1%), thymidine analog mutations (29.6%), Y181CY (22.2%). The pattern of mutations did not always correspond to the ongoing treatment. The adjusted odds of VF was significantly associated with the decentralized clinic site (<i>P</i> < .001) and CD4 < 350 cells/mm<sup>3</sup> (<i>P</i> < .006). Strong correlates of DR also included Saint-Louis (<i>P</i> < .009), CD4 < 350 cells/mm<sup>3</sup> (<i>P</i> <. 001), and nevirapine-based therapies (comparator: efavirenz-based therapies; <i>P</i> < .027). In stratification analyses by site, higher rate of VF at Saint-Louis (20.5% [95%CI: 13.8-28.5] vs 4.0% [95%CI: 1.5-8.5] in Dakar) was associated with nevirapine-based therapies (OR = 3.34 [1.07-11.75], <i>P</i> = .038), self-reported missing doses (OR = 3.30 [1.13-10.24], <i>P</i> = .029), and medical appointments (OR = 2.91 [1.05-8.47], <i>P</i> = .039) in the last 1 and 12 months(s), respectively. The higher rate of DR at Saint-Louis (12.9% [95%CI: 7.6-20.1] vs 2.7% [95%CI: 0.7-6.7] in Dakar) was associated with nevirapine-based therapies (OR = 5.13 [1.12-37.35], <i>P</i> = .035).</p><p><strong>Conclusion: </strong>At decentralized urban settings, there is need for enhanced virological monitoring and adherence support. HIV programs in Senegal should intensify early HIV diagnosis for effective test-and-treat. These interventions, in addition to the superiority of efavirenz-based therapies provide a favorable framework for transitioning to the recommended potent drug dolutegravir, thereby ensuring its long-term use.</p>\",\"PeriodicalId\":13671,\"journal\":{\"name\":\"Infectious Diseases\",\"volume\":\"14 \",\"pages\":\"11786337211014503\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2021-05-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/aa/d3/10.1177_11786337211014503.PMC8120520.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/11786337211014503\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/11786337211014503","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
摘要
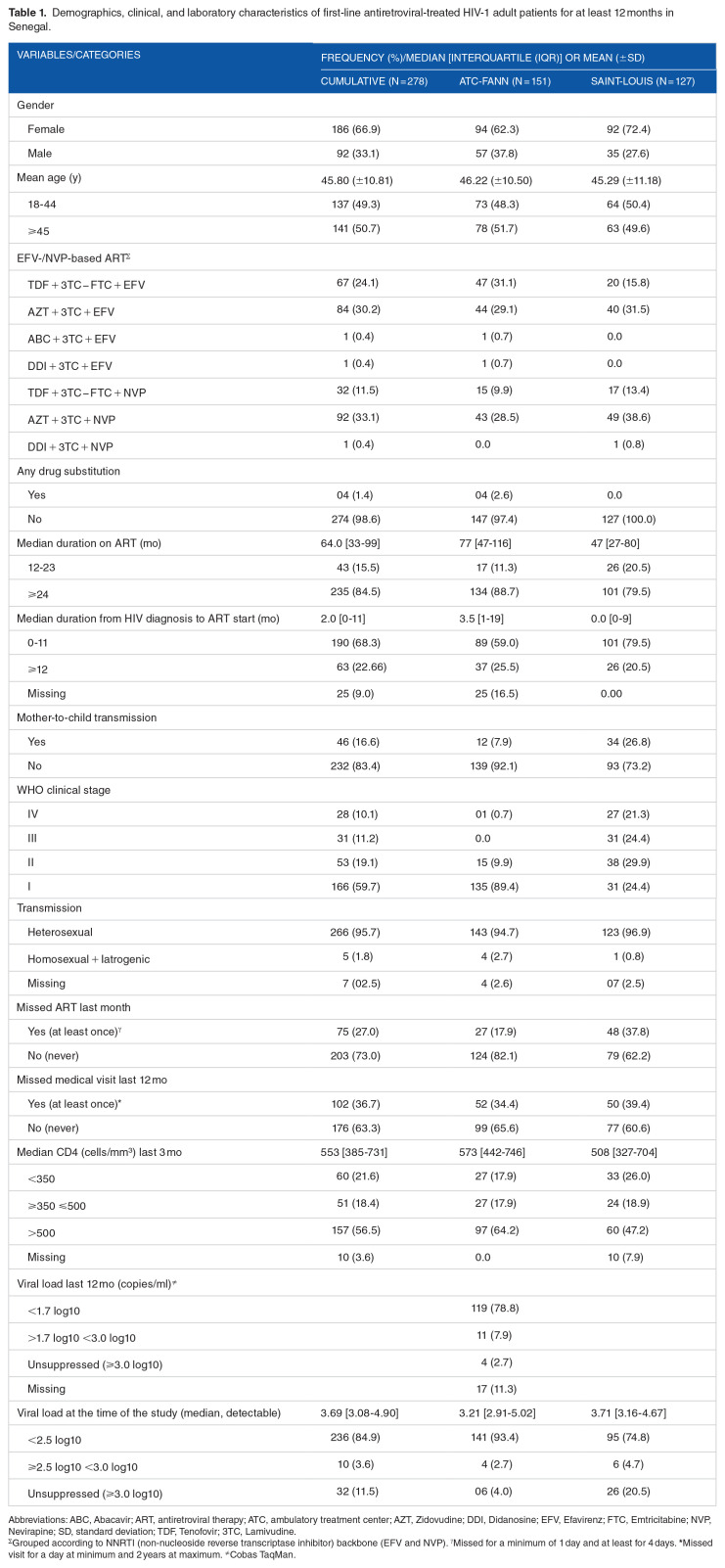
背景:在撒哈拉以南非洲分散的 HIV 诊所中,抗逆转录病毒疗法(ART)监测的可行性仍然存在问题。我们评估了塞内加尔两个先测后治的城市诊所中 HIV-1 病毒学失败(VF)和耐药性(DR)的发生率及相关因素:2015年1月至3月期间,在达喀尔转诊门诊治疗中心(n = 151)和圣路易分散地区医院(n = 127)对同意接受一线抗逆转录病毒疗法达12个月的HIV-1感染成人(⩾18岁)进行了横断面登记。在采集血浆标本之前的12个月中,圣路易医院的患者未进行病毒载量(VL)检测。使用 R 软件中的二项式逻辑回归法确定了 VF(VL ⩾ 1000拷贝/毫升)和 DR(临床相关突变)的重要预测因素:在接受以 EFV/NVP 为基础的治疗方案的 278 名成人中,有 32 人(11.5% [95%CI:8.0-15.9])出现 VF。失败和非失败患者接受抗逆转录病毒疗法的中位时间[四分位间]相当(69.5 [23.0-89.5] vs 64.0 [34.0-99.0] 个月;P = .46,Mann-Whitney U 检验)。在成功进行基因分型的 27 个病毒分离株中,20 个(74.1%)携带 DR 变异;最常见的是 M184VI(55.6%)、K103N(37.1%)、胸腺嘧啶类似物突变(29.6%)和 Y181CY(22.2%)。突变的模式并不总是与正在进行的治疗相对应。调整后的 VF 发生几率分别与过去 1 个月和 12 个月的分散诊所地点(P 3 (P P 3 (P P P = .038))、自我报告的缺失剂量(OR = 3.30 [1.13-10.24],P = .029)和医疗预约(OR = 2.91 [1.05-8.47],P = .039)显著相关。圣路易的 DR 发生率较高(12.9% [95%CI: 7.6-20.1] vs 达喀尔的 2.7% [95%CI: 0.7-6.7]),与奈韦拉平疗法有关(OR = 5.13 [1.12-37.35],P = .035):结论:在分散的城市环境中,需要加强病毒学监测和依从性支持。塞内加尔的艾滋病项目应加强早期艾滋病诊断,以实现有效的检测和治疗。这些干预措施以及以依非韦伦为基础的疗法的优越性为过渡到推荐的强效药物多鲁曲韦提供了有利的框架,从而确保其长期使用。
High HIV-1 Virological Failure and Drug Resistance among Adult Patients Receiving First-Line ART for At least 12 Months at a Decentralized Urban HIV Clinic Setting in Senegal before the Test-and-Treat.
Background: The feasibility of antiretroviral therapy (ART) monitoring remains problematic in decentralized HIV clinic settings of sub-Saharan Africa. We assessed the rates and correlates of HIV-1 virological failure (VF) and drug resistance (DR) in 2 pre-test-and-treat urban clinic settings of Senegal.
Methods: Consenting HIV-1-infected adults (⩾18 years) receiving first-line ART for ⩾12 months were cross-sectionally enrolled between January and March 2015, at the referral outpatient treatment center of Dakar (n = 151) and decentralized regional hospital of Saint-Louis (n = 127). In the 12 months preceding plasma specimens' collection patients at Saint-Louis had no viral load (VL) testing. Significant predictors of VF (VL ⩾ 1000 copies/ml) and DR (clinically relevant mutations) were determined using binomial logistic regression in R software.
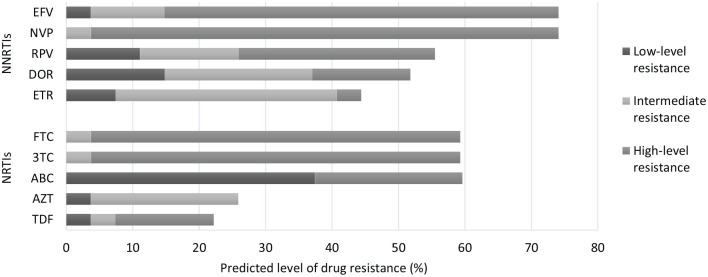
Results: Of the 278 adults on EFV-/NVP-based regimens, 32 (11.5% [95%CI: 8.0-15.9]) experienced VF. Failing and non-failing patients had comparable median time [interquartile] on ART (69.5 [23.0-89.5] vs 64.0 [34.0-99.0] months; P = .46, Mann-Whitney U-test). Of the 27 viraemic isolates successfully genotyped, 20 (74.1%) carried DR mutations; most frequent were M184VI (55.6%), K103N (37.1%), thymidine analog mutations (29.6%), Y181CY (22.2%). The pattern of mutations did not always correspond to the ongoing treatment. The adjusted odds of VF was significantly associated with the decentralized clinic site (P < .001) and CD4 < 350 cells/mm3 (P < .006). Strong correlates of DR also included Saint-Louis (P < .009), CD4 < 350 cells/mm3 (P <. 001), and nevirapine-based therapies (comparator: efavirenz-based therapies; P < .027). In stratification analyses by site, higher rate of VF at Saint-Louis (20.5% [95%CI: 13.8-28.5] vs 4.0% [95%CI: 1.5-8.5] in Dakar) was associated with nevirapine-based therapies (OR = 3.34 [1.07-11.75], P = .038), self-reported missing doses (OR = 3.30 [1.13-10.24], P = .029), and medical appointments (OR = 2.91 [1.05-8.47], P = .039) in the last 1 and 12 months(s), respectively. The higher rate of DR at Saint-Louis (12.9% [95%CI: 7.6-20.1] vs 2.7% [95%CI: 0.7-6.7] in Dakar) was associated with nevirapine-based therapies (OR = 5.13 [1.12-37.35], P = .035).
Conclusion: At decentralized urban settings, there is need for enhanced virological monitoring and adherence support. HIV programs in Senegal should intensify early HIV diagnosis for effective test-and-treat. These interventions, in addition to the superiority of efavirenz-based therapies provide a favorable framework for transitioning to the recommended potent drug dolutegravir, thereby ensuring its long-term use.
期刊介绍:
Infectious Diseases (formerly Scandinavian Journal of Infectious Diseases) is a peer-reviewed journal publishing articles on all aspects of human infection, including pathogenesis, diagnosis, and treatment of infectious diseases, and also on medical microbiology and epidemiology

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


