Na Xiao, Hailang He, Jing Wang, Li Zhang, Brandon Chow, Fanchao Feng, Yong Xu, Jingyi Huang, Xianmei Zhou, Rui Dong
{"title":"爱地注射液与第一代表皮生长因子受体-酪氨酸激酶抑制剂治疗晚期非小细胞肺癌的meta分析。","authors":"Na Xiao, Hailang He, Jing Wang, Li Zhang, Brandon Chow, Fanchao Feng, Yong Xu, Jingyi Huang, Xianmei Zhou, Rui Dong","doi":"10.1177/2515690X211010733","DOIUrl":null,"url":null,"abstract":"<p><p>The combination of Aidi injection (ADI) and epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) in treating non-small cell lung cancer (NSCLC) has been reported, but the effects of this therapy have not been systematically assessed. Randomized controlled trials (RCTs) published before June 2020 were searched from 6 databases. Two reviewers independently assessed the methodological quality of 8 RCTs involving 667 patients diagnosed with stage III-IV NSCLC. We found that ADI combined with EGFR-TKI increased the objective response rate (ORR) significantly (relative risk [RR]: 1.60; 95% confidence interval [CI]: 1.28-1.99, <i>P</i> < 0.0001). There was also improvement in the disease control rate (DCR) (RR: 1.25; 95% CI: 1.11-1.40, <i>P</i> = 0.0002) as compared with EGFR-TKI alone. This therapy also increased the percentage of CD3<sup>+</sup> cells (weighted mean difference [WMD]: 9.86; 95% CI: 4.62-15.10), CD4<sup>+</sup> cells (WMD: 6.10; 95% CI: 1.67-10.53), and the CD4<sup>+</sup>/CD8<sup>+</sup> (WMD: 0.35; 95% CI: 0.28-0.43). With regard to drug toxicity, the occurrence of rash was significantly reduced by ADI combined with EGFR-TKI (RR: 0.78, 95% CI: 0.63-0.97, <i>P</i> = 0.03); however, we did not find a significant reduction in the occurrence of dry skin, nausea and vomiting, as well as diarrhea between the 2 therapies. ADI combined with first-generation EGFR-TKIs may be more effective in improving tumor response, reducing the occurrence of rash, and enhancing immune function in NSCLC than EGFR-TKI alone.</p>","PeriodicalId":15714,"journal":{"name":"Journal of Evidence-based Integrative Medicine","volume":"26 ","pages":"2515690X211010733"},"PeriodicalIF":3.3000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2515690X211010733","citationCount":"1","resultStr":"{\"title\":\"Meta-Analysis of Aidi Injection and First-Generation Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor Therapy in Treating Advanced Non-Small Cell Lung Cancer.\",\"authors\":\"Na Xiao, Hailang He, Jing Wang, Li Zhang, Brandon Chow, Fanchao Feng, Yong Xu, Jingyi Huang, Xianmei Zhou, Rui Dong\",\"doi\":\"10.1177/2515690X211010733\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The combination of Aidi injection (ADI) and epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) in treating non-small cell lung cancer (NSCLC) has been reported, but the effects of this therapy have not been systematically assessed. Randomized controlled trials (RCTs) published before June 2020 were searched from 6 databases. Two reviewers independently assessed the methodological quality of 8 RCTs involving 667 patients diagnosed with stage III-IV NSCLC. We found that ADI combined with EGFR-TKI increased the objective response rate (ORR) significantly (relative risk [RR]: 1.60; 95% confidence interval [CI]: 1.28-1.99, <i>P</i> < 0.0001). There was also improvement in the disease control rate (DCR) (RR: 1.25; 95% CI: 1.11-1.40, <i>P</i> = 0.0002) as compared with EGFR-TKI alone. This therapy also increased the percentage of CD3<sup>+</sup> cells (weighted mean difference [WMD]: 9.86; 95% CI: 4.62-15.10), CD4<sup>+</sup> cells (WMD: 6.10; 95% CI: 1.67-10.53), and the CD4<sup>+</sup>/CD8<sup>+</sup> (WMD: 0.35; 95% CI: 0.28-0.43). With regard to drug toxicity, the occurrence of rash was significantly reduced by ADI combined with EGFR-TKI (RR: 0.78, 95% CI: 0.63-0.97, <i>P</i> = 0.03); however, we did not find a significant reduction in the occurrence of dry skin, nausea and vomiting, as well as diarrhea between the 2 therapies. ADI combined with first-generation EGFR-TKIs may be more effective in improving tumor response, reducing the occurrence of rash, and enhancing immune function in NSCLC than EGFR-TKI alone.</p>\",\"PeriodicalId\":15714,\"journal\":{\"name\":\"Journal of Evidence-based Integrative Medicine\",\"volume\":\"26 \",\"pages\":\"2515690X211010733\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/2515690X211010733\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Evidence-based Integrative Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2515690X211010733\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"INTEGRATIVE & COMPLEMENTARY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Evidence-based Integrative Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2515690X211010733","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INTEGRATIVE & COMPLEMENTARY MEDICINE","Score":null,"Total":0}
Meta-Analysis of Aidi Injection and First-Generation Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor Therapy in Treating Advanced Non-Small Cell Lung Cancer.
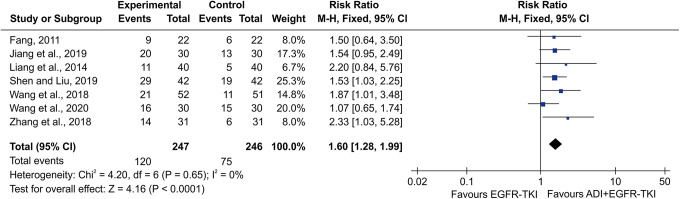
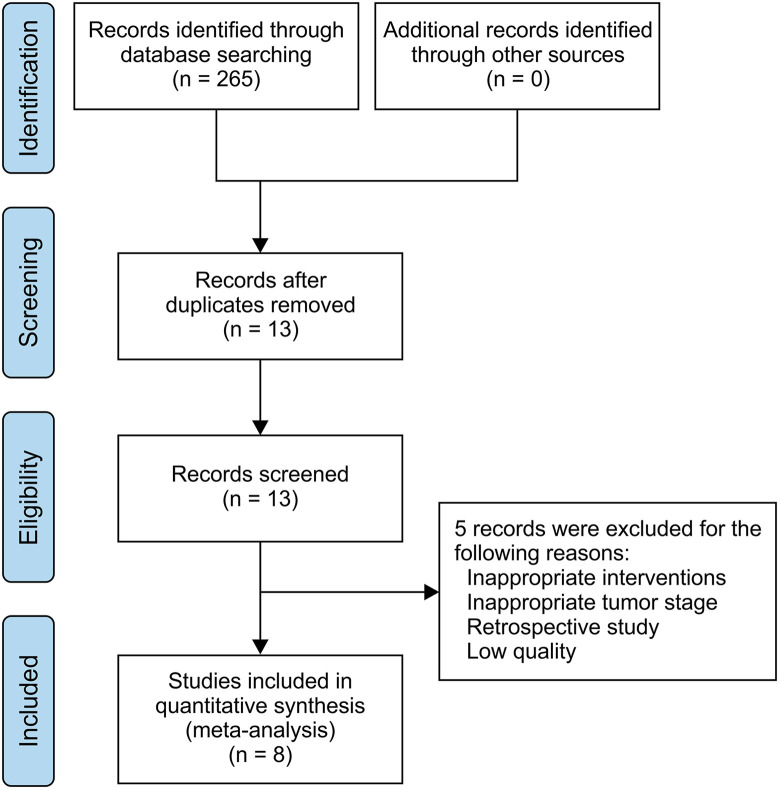
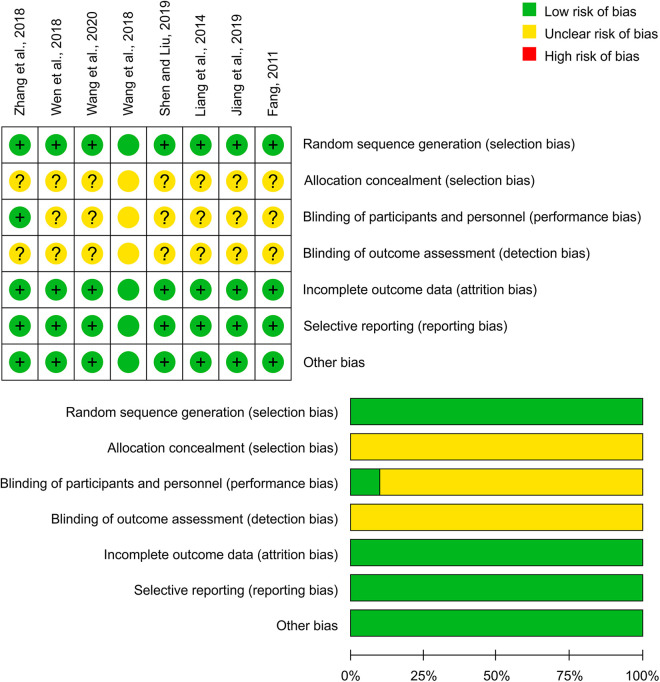
The combination of Aidi injection (ADI) and epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) in treating non-small cell lung cancer (NSCLC) has been reported, but the effects of this therapy have not been systematically assessed. Randomized controlled trials (RCTs) published before June 2020 were searched from 6 databases. Two reviewers independently assessed the methodological quality of 8 RCTs involving 667 patients diagnosed with stage III-IV NSCLC. We found that ADI combined with EGFR-TKI increased the objective response rate (ORR) significantly (relative risk [RR]: 1.60; 95% confidence interval [CI]: 1.28-1.99, P < 0.0001). There was also improvement in the disease control rate (DCR) (RR: 1.25; 95% CI: 1.11-1.40, P = 0.0002) as compared with EGFR-TKI alone. This therapy also increased the percentage of CD3+ cells (weighted mean difference [WMD]: 9.86; 95% CI: 4.62-15.10), CD4+ cells (WMD: 6.10; 95% CI: 1.67-10.53), and the CD4+/CD8+ (WMD: 0.35; 95% CI: 0.28-0.43). With regard to drug toxicity, the occurrence of rash was significantly reduced by ADI combined with EGFR-TKI (RR: 0.78, 95% CI: 0.63-0.97, P = 0.03); however, we did not find a significant reduction in the occurrence of dry skin, nausea and vomiting, as well as diarrhea between the 2 therapies. ADI combined with first-generation EGFR-TKIs may be more effective in improving tumor response, reducing the occurrence of rash, and enhancing immune function in NSCLC than EGFR-TKI alone.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


