Niraj Desai, Brigid Wilson, Michael Bond, Alexander Conant, Mahboob Rahman
{"title":"有或无慢性肾脏疾病的ALLHAT参与者阿司匹林使用与心血管结局的关系:事后分析","authors":"Niraj Desai, Brigid Wilson, Michael Bond, Alexander Conant, Mahboob Rahman","doi":"10.1111/jch.14091","DOIUrl":null,"url":null,"abstract":"<p><p>It is unclear whether aspirin is beneficial for prevention of CVD in patients with CKD. We performed a secondary analysis of the ALLHAT trial to assess the effect of baseline aspirin use on nonfatal myocardial infarction (MI) or fatal coronary heart disease (CHD), all-cause mortality, and stroke. Baseline characteristics of aspirin users and nonusers were used to generate propensity-matched cohorts. Using conditional Cox proportional hazard regression models, we examined the effect of aspirin on the outcomes in the cohort at large and across 3 levels of kidney function (eGFR ≥90, 60-89, and <60). 11 250 ALLHAT participants reported using aspirin at baseline. The propensity-matched dataset included 6894 nonusers matched with replacement to achieve a balanced analysis population (n = 22 500). Risk of fatal CHD or nonfatal MI (HR = 0.94, 95% CI 0.86-1.02) and stroke (HR = 1.01, 95% CI 0.89-1.15) was not significantly different between groups. Aspirin users were at significantly lower risk of all-cause mortality compared to nonusers (HR = 0.82, 95% CI 0.76-0.88). Aspirin use was not associated with incidence of fatal CAD or nonfatal MI in patients with CVD (HR = 0.93, CI 0.84-1.04) or without CVD at baseline (HR = 1.04, CI 0.82-1.32). Results were consistent across strata of GFR (interaction p value NS). In hypertensive patients at high cardiovascular risk, aspirin use is not associated with risk of nonfatal MI, fatal CHD, or stroke; however, aspirin use is associated with lower risk of all-cause mortality. These results are consistent across baseline eGFR.</p>","PeriodicalId":520663,"journal":{"name":"Journal of clinical hypertension (Greenwich, Conn.)","volume":" ","pages":"352-362"},"PeriodicalIF":2.5000,"publicationDate":"2021-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1111/jch.14091","citationCount":"3","resultStr":"{\"title\":\"Association between aspirin use and cardiovascular outcomes in ALLHAT participants with and without chronic kidney disease: A post hoc analysis.\",\"authors\":\"Niraj Desai, Brigid Wilson, Michael Bond, Alexander Conant, Mahboob Rahman\",\"doi\":\"10.1111/jch.14091\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>It is unclear whether aspirin is beneficial for prevention of CVD in patients with CKD. We performed a secondary analysis of the ALLHAT trial to assess the effect of baseline aspirin use on nonfatal myocardial infarction (MI) or fatal coronary heart disease (CHD), all-cause mortality, and stroke. Baseline characteristics of aspirin users and nonusers were used to generate propensity-matched cohorts. Using conditional Cox proportional hazard regression models, we examined the effect of aspirin on the outcomes in the cohort at large and across 3 levels of kidney function (eGFR ≥90, 60-89, and <60). 11 250 ALLHAT participants reported using aspirin at baseline. The propensity-matched dataset included 6894 nonusers matched with replacement to achieve a balanced analysis population (n = 22 500). Risk of fatal CHD or nonfatal MI (HR = 0.94, 95% CI 0.86-1.02) and stroke (HR = 1.01, 95% CI 0.89-1.15) was not significantly different between groups. Aspirin users were at significantly lower risk of all-cause mortality compared to nonusers (HR = 0.82, 95% CI 0.76-0.88). Aspirin use was not associated with incidence of fatal CAD or nonfatal MI in patients with CVD (HR = 0.93, CI 0.84-1.04) or without CVD at baseline (HR = 1.04, CI 0.82-1.32). Results were consistent across strata of GFR (interaction p value NS). In hypertensive patients at high cardiovascular risk, aspirin use is not associated with risk of nonfatal MI, fatal CHD, or stroke; however, aspirin use is associated with lower risk of all-cause mortality. These results are consistent across baseline eGFR.</p>\",\"PeriodicalId\":520663,\"journal\":{\"name\":\"Journal of clinical hypertension (Greenwich, Conn.)\",\"volume\":\" \",\"pages\":\"352-362\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2021-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1111/jch.14091\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of clinical hypertension (Greenwich, Conn.)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/jch.14091\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/12/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical hypertension (Greenwich, Conn.)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/jch.14091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/12/19 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Association between aspirin use and cardiovascular outcomes in ALLHAT participants with and without chronic kidney disease: A post hoc analysis.
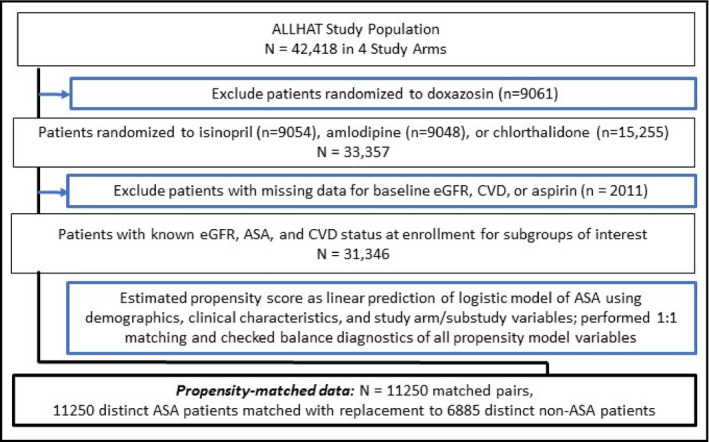
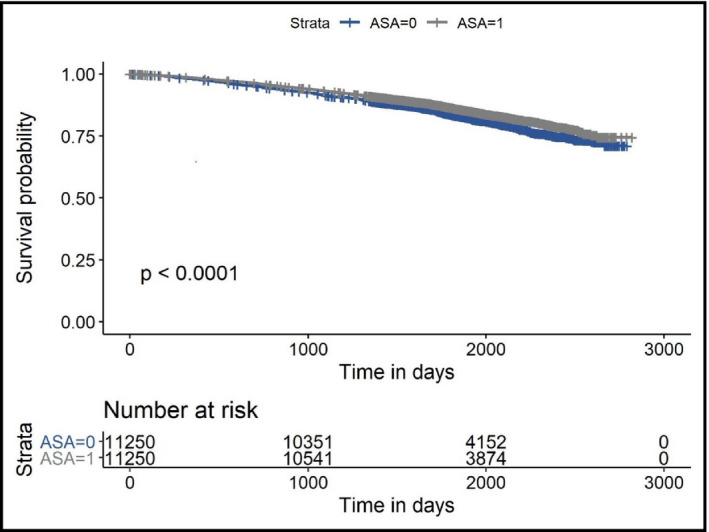
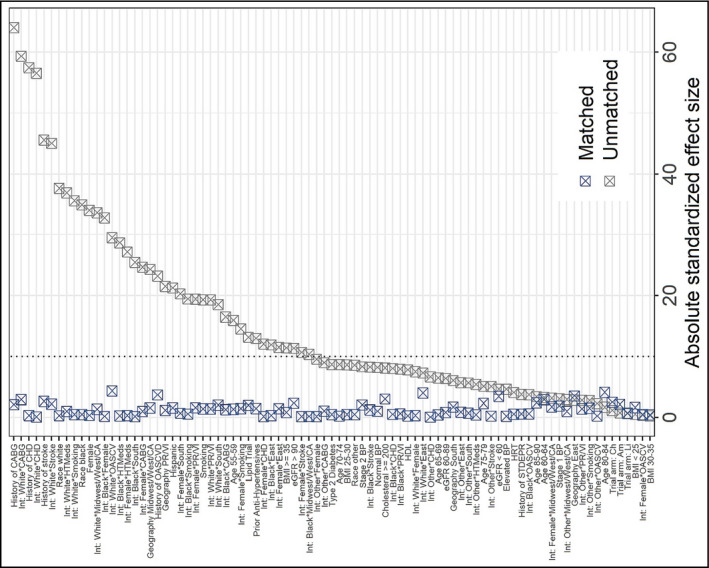
It is unclear whether aspirin is beneficial for prevention of CVD in patients with CKD. We performed a secondary analysis of the ALLHAT trial to assess the effect of baseline aspirin use on nonfatal myocardial infarction (MI) or fatal coronary heart disease (CHD), all-cause mortality, and stroke. Baseline characteristics of aspirin users and nonusers were used to generate propensity-matched cohorts. Using conditional Cox proportional hazard regression models, we examined the effect of aspirin on the outcomes in the cohort at large and across 3 levels of kidney function (eGFR ≥90, 60-89, and <60). 11 250 ALLHAT participants reported using aspirin at baseline. The propensity-matched dataset included 6894 nonusers matched with replacement to achieve a balanced analysis population (n = 22 500). Risk of fatal CHD or nonfatal MI (HR = 0.94, 95% CI 0.86-1.02) and stroke (HR = 1.01, 95% CI 0.89-1.15) was not significantly different between groups. Aspirin users were at significantly lower risk of all-cause mortality compared to nonusers (HR = 0.82, 95% CI 0.76-0.88). Aspirin use was not associated with incidence of fatal CAD or nonfatal MI in patients with CVD (HR = 0.93, CI 0.84-1.04) or without CVD at baseline (HR = 1.04, CI 0.82-1.32). Results were consistent across strata of GFR (interaction p value NS). In hypertensive patients at high cardiovascular risk, aspirin use is not associated with risk of nonfatal MI, fatal CHD, or stroke; however, aspirin use is associated with lower risk of all-cause mortality. These results are consistent across baseline eGFR.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


