Samuel T Montgomery, Stephen M Stick, Anthony Kicic
{"title":"一种适应的新型流式细胞术方法来描述气道上皮细胞的细胞死亡类型。","authors":"Samuel T Montgomery, Stephen M Stick, Anthony Kicic","doi":"10.14440/jbm.2020.336","DOIUrl":null,"url":null,"abstract":"<p><p>Current methodologies to measure apoptotic and necrotic cell death using flow cytometry do not adequately differentiate between the two. Here, we describe a flow cytometry methodology adapted to airway epithelial cells (AEC) to sufficiently differentiate apoptotic and necrotic AEC. Specifically, cell lines and primary AEC (<i>n</i> = 12) were permeabilized or infected with rhinovirus 1b (RV1b) over 48 h. Cell death was then measured <i>via</i> annexin V/propidium iodide (A5/PI) or annexin V/TO-PRO-3 (A5/TP3) staining using a novel flow cytometry and gating methodology adapted to AEC. We show that A5/PI staining could not sufficiently differentiate between types of cell death following RV1b infection of primary AEC. However, A5/TP3 staining was able to distinguish six cell death populations (viable, necrotic, debris, A5<sup>+</sup> apoptotic, A5<sup>-</sup> apoptotic, apoptotic bodies) after permeabilization or infection with RV1b, with phenotypic differences were observed in apoptotic populations. Collectively, using a staining and gating strategy never adapted to AEC, A5/TP3 could accurately differentiate and quantify viable, necrotic, and apoptotic AEC following RV1b infection.</p>","PeriodicalId":73618,"journal":{"name":"Journal of biological methods","volume":" ","pages":"e139"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cd/b1/jbm-7-4-e139.PMC7666329.pdf","citationCount":"1","resultStr":"{\"title\":\"An adapted novel flow cytometry methodology to delineate types of cell death in airway epithelial cells.\",\"authors\":\"Samuel T Montgomery, Stephen M Stick, Anthony Kicic\",\"doi\":\"10.14440/jbm.2020.336\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Current methodologies to measure apoptotic and necrotic cell death using flow cytometry do not adequately differentiate between the two. Here, we describe a flow cytometry methodology adapted to airway epithelial cells (AEC) to sufficiently differentiate apoptotic and necrotic AEC. Specifically, cell lines and primary AEC (<i>n</i> = 12) were permeabilized or infected with rhinovirus 1b (RV1b) over 48 h. Cell death was then measured <i>via</i> annexin V/propidium iodide (A5/PI) or annexin V/TO-PRO-3 (A5/TP3) staining using a novel flow cytometry and gating methodology adapted to AEC. We show that A5/PI staining could not sufficiently differentiate between types of cell death following RV1b infection of primary AEC. However, A5/TP3 staining was able to distinguish six cell death populations (viable, necrotic, debris, A5<sup>+</sup> apoptotic, A5<sup>-</sup> apoptotic, apoptotic bodies) after permeabilization or infection with RV1b, with phenotypic differences were observed in apoptotic populations. Collectively, using a staining and gating strategy never adapted to AEC, A5/TP3 could accurately differentiate and quantify viable, necrotic, and apoptotic AEC following RV1b infection.</p>\",\"PeriodicalId\":73618,\"journal\":{\"name\":\"Journal of biological methods\",\"volume\":\" \",\"pages\":\"e139\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-11-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cd/b1/jbm-7-4-e139.PMC7666329.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of biological methods\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14440/jbm.2020.336\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of biological methods","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14440/jbm.2020.336","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
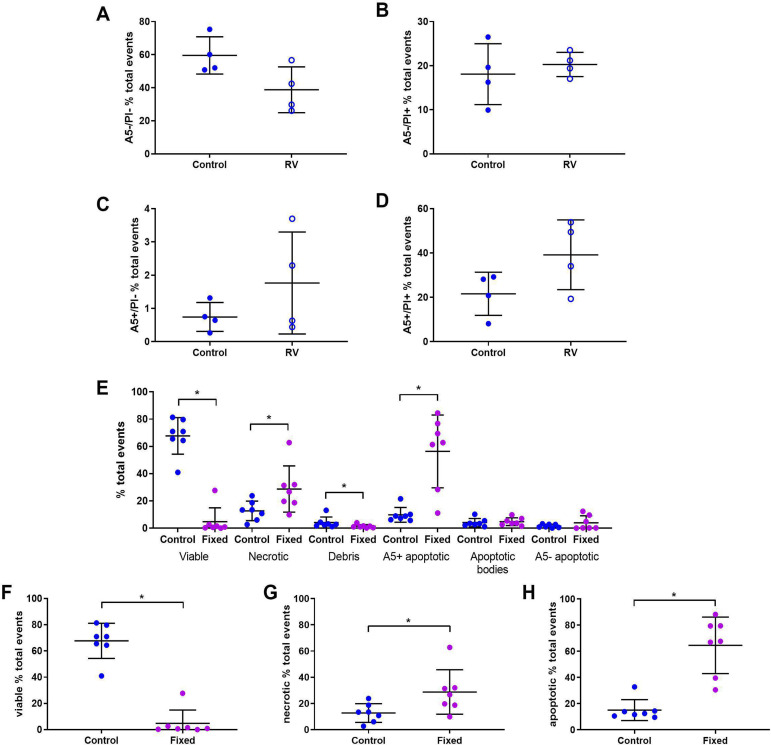
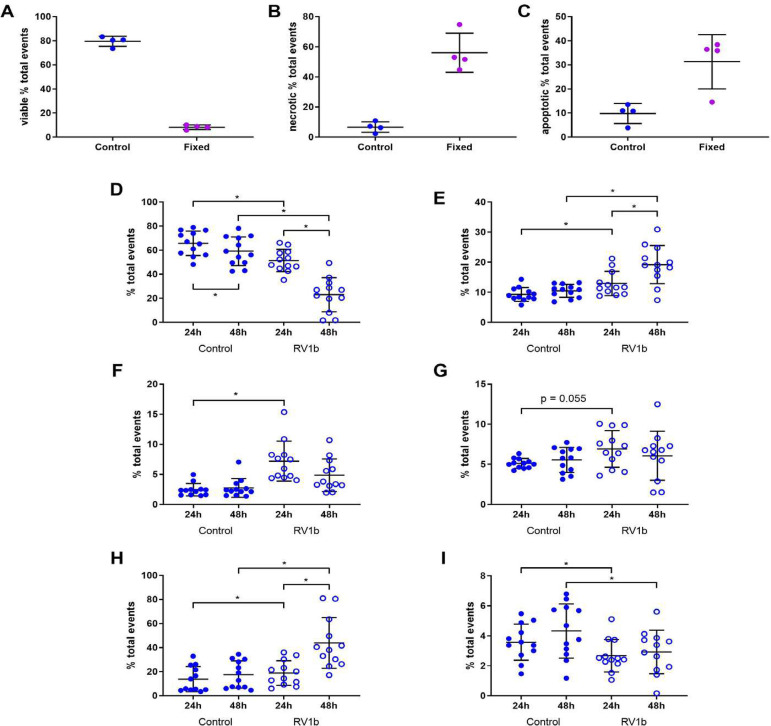
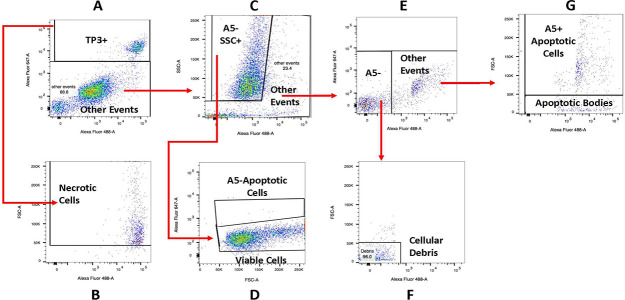
目前使用流式细胞术测量凋亡和坏死细胞死亡的方法不能充分区分两者。在这里,我们描述了一种适用于气道上皮细胞(AEC)的流式细胞术方法,以充分区分凋亡和坏死的AEC。具体来说,细胞系和原代AEC (n = 12)在48小时内被鼻病毒1b (RV1b)渗透或感染。然后使用适用于AEC的新型流式细胞术和门控方法,通过膜联蛋白V/碘化丙啶(A5/PI)或膜联蛋白V/ to - pro -3 (A5/TP3)染色来测量细胞死亡。我们发现A5/PI染色不能充分区分RV1b感染原发AEC后细胞死亡的类型。然而,A5/TP3染色能够区分透性或感染RV1b后的6种细胞死亡群体(活细胞、坏死细胞、碎片细胞、A5+凋亡细胞、A5-凋亡细胞、凋亡小体细胞),凋亡群体之间存在表型差异。总的来说,使用从未适应于AEC的染色和门控策略,A5/TP3可以准确地区分和量化RV1b感染后的活的、坏死的和凋亡的AEC。
An adapted novel flow cytometry methodology to delineate types of cell death in airway epithelial cells.
Current methodologies to measure apoptotic and necrotic cell death using flow cytometry do not adequately differentiate between the two. Here, we describe a flow cytometry methodology adapted to airway epithelial cells (AEC) to sufficiently differentiate apoptotic and necrotic AEC. Specifically, cell lines and primary AEC (n = 12) were permeabilized or infected with rhinovirus 1b (RV1b) over 48 h. Cell death was then measured via annexin V/propidium iodide (A5/PI) or annexin V/TO-PRO-3 (A5/TP3) staining using a novel flow cytometry and gating methodology adapted to AEC. We show that A5/PI staining could not sufficiently differentiate between types of cell death following RV1b infection of primary AEC. However, A5/TP3 staining was able to distinguish six cell death populations (viable, necrotic, debris, A5+ apoptotic, A5- apoptotic, apoptotic bodies) after permeabilization or infection with RV1b, with phenotypic differences were observed in apoptotic populations. Collectively, using a staining and gating strategy never adapted to AEC, A5/TP3 could accurately differentiate and quantify viable, necrotic, and apoptotic AEC following RV1b infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


