David Maskill, Janice Hoole, Katerina Oikonomi, Ian Simmons, Evangelos Drimtzias
{"title":"重度重眼综合征双侧无增强环形近视手术一例。","authors":"David Maskill, Janice Hoole, Katerina Oikonomi, Ian Simmons, Evangelos Drimtzias","doi":"10.22599/bioj.125","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To report the clinical features and surgical outcomes of one patient with heavy eye syndrome who underwent bilateral, unaugmented, full loop myopexy.</p><p><strong>Methods: </strong>A 47-year-old lady with high myopia, high axial length, progressive esotropia, slippage of the lateral rectus (LR) inferiorly and superior rectus (SR) medially on magnetic resonance imaging (MRI) was diagnosed with heavy eye syndrome. Unaugmented loop myopexy without medial rectus (MR) recession was offered.</p><p><strong>Results: </strong>On follow-up at 30 months, a small residual esotropia of 6 prism diopters (PD) at near and 10 PD at distance was achieved. Both abduction and elevation were improved in both eyes.</p><p><strong>Conclusions: </strong>The high angle of esodeviation can be challenging to correct adequately with surgery, with many options available: resection-recession, hemitranspositions (Yamada's procedure), partial loop myopexy (modified Jensen's procedure) and full loop myopexy (Yokoyama's procedure). It remains unclear which procedure is optimal for severe disease. In this case, we present bilateral, unaugmented, full loop myopexy as our preferred choice for high esotropia.</p>","PeriodicalId":36083,"journal":{"name":"British and Irish Orthoptic Journal","volume":"15 1","pages":"25-27"},"PeriodicalIF":0.0000,"publicationDate":"2019-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7510404/pdf/","citationCount":"0","resultStr":"{\"title\":\"Bilateral, Unaugmented, Loop Myopexy Performed for a Severe Case of Heavy Eye Syndrome.\",\"authors\":\"David Maskill, Janice Hoole, Katerina Oikonomi, Ian Simmons, Evangelos Drimtzias\",\"doi\":\"10.22599/bioj.125\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>To report the clinical features and surgical outcomes of one patient with heavy eye syndrome who underwent bilateral, unaugmented, full loop myopexy.</p><p><strong>Methods: </strong>A 47-year-old lady with high myopia, high axial length, progressive esotropia, slippage of the lateral rectus (LR) inferiorly and superior rectus (SR) medially on magnetic resonance imaging (MRI) was diagnosed with heavy eye syndrome. Unaugmented loop myopexy without medial rectus (MR) recession was offered.</p><p><strong>Results: </strong>On follow-up at 30 months, a small residual esotropia of 6 prism diopters (PD) at near and 10 PD at distance was achieved. Both abduction and elevation were improved in both eyes.</p><p><strong>Conclusions: </strong>The high angle of esodeviation can be challenging to correct adequately with surgery, with many options available: resection-recession, hemitranspositions (Yamada's procedure), partial loop myopexy (modified Jensen's procedure) and full loop myopexy (Yokoyama's procedure). It remains unclear which procedure is optimal for severe disease. In this case, we present bilateral, unaugmented, full loop myopexy as our preferred choice for high esotropia.</p>\",\"PeriodicalId\":36083,\"journal\":{\"name\":\"British and Irish Orthoptic Journal\",\"volume\":\"15 1\",\"pages\":\"25-27\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-02-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7510404/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"British and Irish Orthoptic Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22599/bioj.125\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"British and Irish Orthoptic Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22599/bioj.125","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Bilateral, Unaugmented, Loop Myopexy Performed for a Severe Case of Heavy Eye Syndrome.
Aim: To report the clinical features and surgical outcomes of one patient with heavy eye syndrome who underwent bilateral, unaugmented, full loop myopexy.
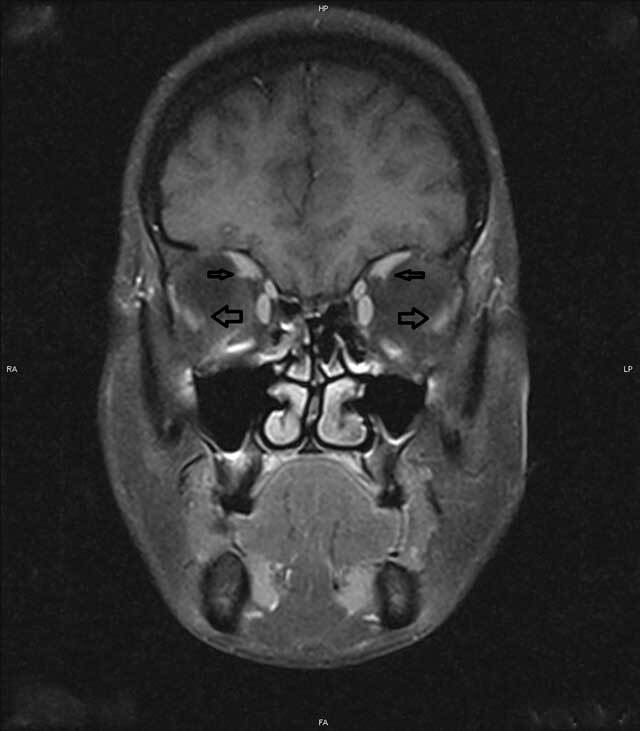
Methods: A 47-year-old lady with high myopia, high axial length, progressive esotropia, slippage of the lateral rectus (LR) inferiorly and superior rectus (SR) medially on magnetic resonance imaging (MRI) was diagnosed with heavy eye syndrome. Unaugmented loop myopexy without medial rectus (MR) recession was offered.
Results: On follow-up at 30 months, a small residual esotropia of 6 prism diopters (PD) at near and 10 PD at distance was achieved. Both abduction and elevation were improved in both eyes.
Conclusions: The high angle of esodeviation can be challenging to correct adequately with surgery, with many options available: resection-recession, hemitranspositions (Yamada's procedure), partial loop myopexy (modified Jensen's procedure) and full loop myopexy (Yokoyama's procedure). It remains unclear which procedure is optimal for severe disease. In this case, we present bilateral, unaugmented, full loop myopexy as our preferred choice for high esotropia.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


