Shah Newaz Ahmed, Ratinder Jhaj, Balakrishnan Sadasivam, Rajnish Joshi
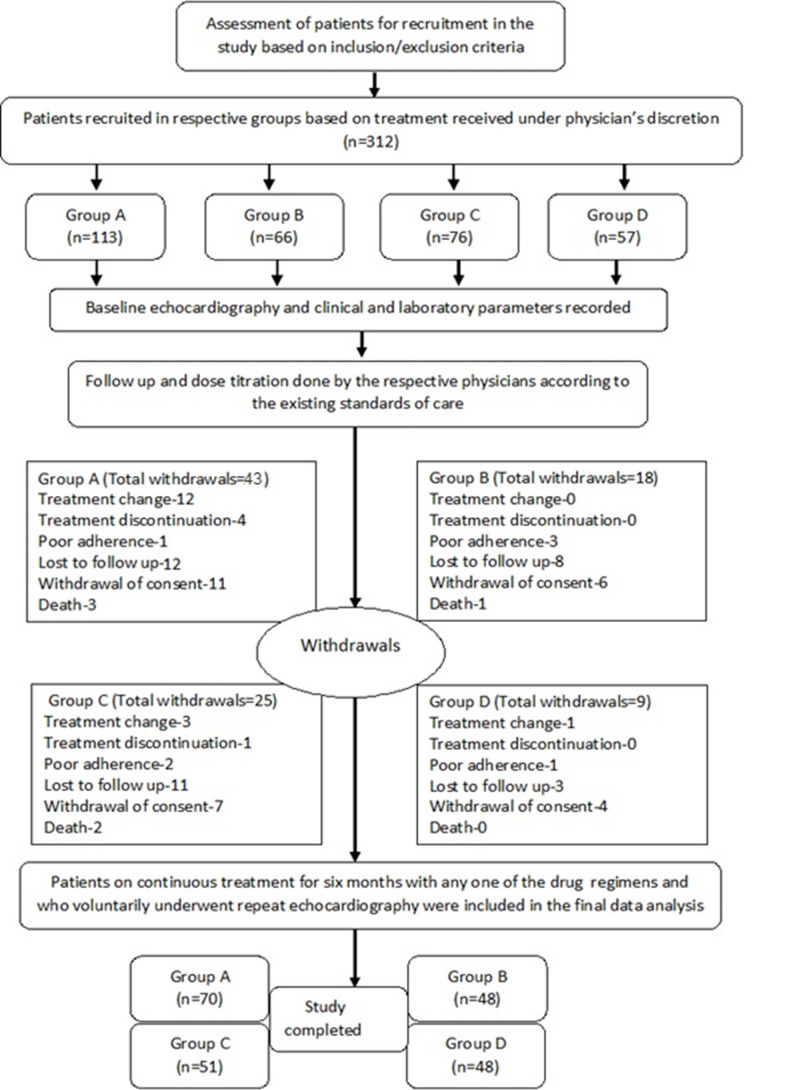
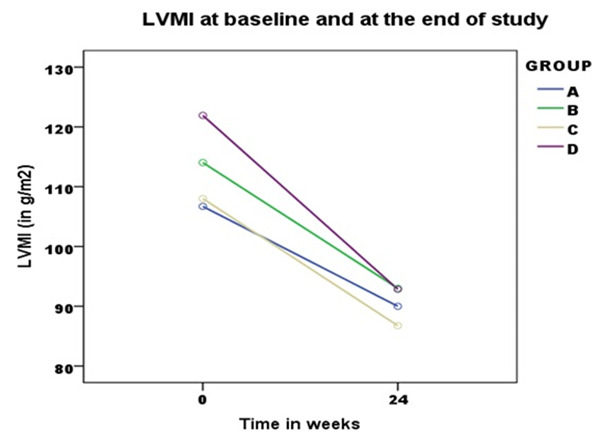
{"title":"标准药物治疗对原发性高血压患者左心室肥厚的消退作用。","authors":"Shah Newaz Ahmed, Ratinder Jhaj, Balakrishnan Sadasivam, Rajnish Joshi","doi":"10.15190/d.2020.12","DOIUrl":null,"url":null,"abstract":"PURPOSE: The American College of Cardiology/ American Heart Association 2017 and European Society of Cardiology/European Society of Hypertension 2018 guidelines were a paradigm shift in hypertension management in contemporary medicine. Lowering of blood pressure to less than 130 (systolic) and 80 (diastolic) mm of Hg irrespective of cardiovascular risk is recommended. While intensive blood pressure control is commonly achievable with rational pharmacotherapy, the magnitude of left ventricular hypertrophy regression is an independent factor in improvement in cardiovascular health. The regression of left ventricular hypertrophy has been adjudged as a clinically useful surrogate marker that reflects the efficacy of hypertension treatment. Though angiotensin converting enzyme inhibitors/ angiotensin receptor blockers (ACEI/ARB) are the preferred initial drug for greater regression of left ventricular mass, the choice of add-on therapy, if required, is still debatable. Therefore, in our observational study, we sought to compare the reduction in left ventricular mass index in hypertensives with left ventricular hypertrophy on standard ACEI/ARB based drug therapy. MATERIALS AND METHODS: The cohort (n=217) comprised of patients with uncontrolled hypertension (blood pressure>140/90 mm of Hg) and left ventricular hypertrophy (left ventricular mass index>115 and 95 gram/square meter in males and females respectively). The add-on drug in ACEI/ARB therapy was either thiazide diuretics (TD) or calcium channel blockers (CCB). Four sub-cohorts were constituted: mono-therapy - group A (n=70, ACEI/ARB), dual-therapy - group B (n=48, ACEI/ARB+TD) and group C (n=51, ACEI/ ARB+CCB), triple therapy - group D (n=48, ACEI/ ARB+TD+CCB). Left ventricular mass index was determined using echocardiography at baseline and after 24 weeks of therapy. RESULTS: There was no significant difference in baseline clinical or demographic variables between group B and group C. Baseline blood pressure and duration of hypertension was greater in group D compared to group A (P<0.001). The reduction in left ventricular mass index (mean ±SD) in the four groups (A to D) was 16.7±18.7, 21.0±20.8, 20.5±15.5 and 29.1±21.5 g/m2 respectively (D>A, P=0.011, B versus C, P=1.00). The corresponding change in blood pressure (systolic/diastolic) was 18.5±13.6/8.9±11.2, 27.5±19.2/12.2±9.3, 23.4±16.7/ 5.4±10.1, 26.6±19.5/10.7±12.8 mm of Hg respectively (systolic, B>A, P=0.027, D>A, P=0.048) (diastolic, B>C, P=0.013). CONCLUSION: Anti-hypertensive treatment with angiotensin converting enzyme inhibitors/angiotensin receptor blockers-based therapy produced graded regression of left ventricular hypertrophy with monotherapy, dual therapy and triple therapy. In dual therapy, add-on of either thiazide diuretics or calcium channel blockers to angiotensin converting enzyme inhibitors/angiotensin receptor blockers showed equal efficacy in regression of left ventricular hypertrophy independent of blood pressure reduction.","PeriodicalId":72829,"journal":{"name":"Discoveries (Craiova, Romania)","volume":"8 3","pages":"e115"},"PeriodicalIF":0.0000,"publicationDate":"2020-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7575414/pdf/","citationCount":"10","resultStr":"{\"title\":\"Regression of the Left Ventricular Hypertrophy in Patients with Essential Hypertension on Standard Drug Therapy.\",\"authors\":\"Shah Newaz Ahmed, Ratinder Jhaj, Balakrishnan Sadasivam, Rajnish Joshi\",\"doi\":\"10.15190/d.2020.12\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"PURPOSE: The American College of Cardiology/ American Heart Association 2017 and European Society of Cardiology/European Society of Hypertension 2018 guidelines were a paradigm shift in hypertension management in contemporary medicine. Lowering of blood pressure to less than 130 (systolic) and 80 (diastolic) mm of Hg irrespective of cardiovascular risk is recommended. While intensive blood pressure control is commonly achievable with rational pharmacotherapy, the magnitude of left ventricular hypertrophy regression is an independent factor in improvement in cardiovascular health. The regression of left ventricular hypertrophy has been adjudged as a clinically useful surrogate marker that reflects the efficacy of hypertension treatment. Though angiotensin converting enzyme inhibitors/ angiotensin receptor blockers (ACEI/ARB) are the preferred initial drug for greater regression of left ventricular mass, the choice of add-on therapy, if required, is still debatable. Therefore, in our observational study, we sought to compare the reduction in left ventricular mass index in hypertensives with left ventricular hypertrophy on standard ACEI/ARB based drug therapy. MATERIALS AND METHODS: The cohort (n=217) comprised of patients with uncontrolled hypertension (blood pressure>140/90 mm of Hg) and left ventricular hypertrophy (left ventricular mass index>115 and 95 gram/square meter in males and females respectively). The add-on drug in ACEI/ARB therapy was either thiazide diuretics (TD) or calcium channel blockers (CCB). Four sub-cohorts were constituted: mono-therapy - group A (n=70, ACEI/ARB), dual-therapy - group B (n=48, ACEI/ARB+TD) and group C (n=51, ACEI/ ARB+CCB), triple therapy - group D (n=48, ACEI/ ARB+TD+CCB). Left ventricular mass index was determined using echocardiography at baseline and after 24 weeks of therapy. RESULTS: There was no significant difference in baseline clinical or demographic variables between group B and group C. Baseline blood pressure and duration of hypertension was greater in group D compared to group A (P<0.001). The reduction in left ventricular mass index (mean ±SD) in the four groups (A to D) was 16.7±18.7, 21.0±20.8, 20.5±15.5 and 29.1±21.5 g/m2 respectively (D>A, P=0.011, B versus C, P=1.00). The corresponding change in blood pressure (systolic/diastolic) was 18.5±13.6/8.9±11.2, 27.5±19.2/12.2±9.3, 23.4±16.7/ 5.4±10.1, 26.6±19.5/10.7±12.8 mm of Hg respectively (systolic, B>A, P=0.027, D>A, P=0.048) (diastolic, B>C, P=0.013). CONCLUSION: Anti-hypertensive treatment with angiotensin converting enzyme inhibitors/angiotensin receptor blockers-based therapy produced graded regression of left ventricular hypertrophy with monotherapy, dual therapy and triple therapy. In dual therapy, add-on of either thiazide diuretics or calcium channel blockers to angiotensin converting enzyme inhibitors/angiotensin receptor blockers showed equal efficacy in regression of left ventricular hypertrophy independent of blood pressure reduction.\",\"PeriodicalId\":72829,\"journal\":{\"name\":\"Discoveries (Craiova, Romania)\",\"volume\":\"8 3\",\"pages\":\"e115\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7575414/pdf/\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Discoveries (Craiova, Romania)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15190/d.2020.12\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Discoveries (Craiova, Romania)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15190/d.2020.12","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
摘要
目的:美国心脏病学会/美国心脏协会2017和欧洲心脏病学会/欧洲高血压学会2018指南是当代医学高血压管理的范式转变。建议将血压降至130(收缩压)和80(舒张压)mmhg以下,而不考虑心血管风险。虽然通过合理的药物治疗通常可以实现强化血压控制,但左心室肥厚消退的程度是心血管健康改善的一个独立因素。左心室肥厚的消退被认为是反映高血压治疗效果的临床有用的替代指标。虽然血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂(ACEI/ARB)是左心室体积更大消退的首选初始药物,但如果需要,选择附加治疗仍然存在争议。因此,在我们的观察性研究中,我们试图比较标准ACEI/ARB药物治疗下左室肥厚的高血压患者左室质量指数的降低。材料与方法:该队列(n=217)由未控制的高血压(血压>140/90 mm Hg)和左心室肥厚(男性和女性左心室质量指数分别>115和95克/平方米)患者组成。ACEI/ARB治疗的附加药物是噻嗪类利尿剂(TD)或钙通道阻滞剂(CCB)。分为4个亚队列:单治疗组A组(n=70, ACEI/ARB),双治疗组B组(n=48, ACEI/ARB+TD)和C组(n=51, ACEI/ARB+ CCB),三联治疗组D组(n=48, ACEI/ARB+TD +CCB)。在基线和治疗24周后用超声心动图测定左心室质量指数。结果:B组和C组的基线临床或人口学变量无显著差异。D组的基线血压和高血压持续时间高于A组(PA, P=0.011; B组比C组,P=1.00)。相应的血压(收缩压/舒张压)变化分别为18.5±13.6/8.9±11.2、27.5±19.2/12.2±9.3、23.4±16.7/ 5.4±10.1、26.6±19.5/10.7±12.8 mm Hg(收缩压,B>A, P=0.027, D>A, P=0.048)(舒张压,B>C, P=0.013)。结论:以血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂为基础的抗高血压治疗,单药、双药和三联治疗均可使左心室肥厚逐渐消退。在双重治疗中,噻嗪类利尿剂或钙通道阻滞剂加用血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂对左心室肥厚的消退具有相同的疗效,而不依赖于血压的降低。
Regression of the Left Ventricular Hypertrophy in Patients with Essential Hypertension on Standard Drug Therapy.
PURPOSE: The American College of Cardiology/ American Heart Association 2017 and European Society of Cardiology/European Society of Hypertension 2018 guidelines were a paradigm shift in hypertension management in contemporary medicine. Lowering of blood pressure to less than 130 (systolic) and 80 (diastolic) mm of Hg irrespective of cardiovascular risk is recommended. While intensive blood pressure control is commonly achievable with rational pharmacotherapy, the magnitude of left ventricular hypertrophy regression is an independent factor in improvement in cardiovascular health. The regression of left ventricular hypertrophy has been adjudged as a clinically useful surrogate marker that reflects the efficacy of hypertension treatment. Though angiotensin converting enzyme inhibitors/ angiotensin receptor blockers (ACEI/ARB) are the preferred initial drug for greater regression of left ventricular mass, the choice of add-on therapy, if required, is still debatable. Therefore, in our observational study, we sought to compare the reduction in left ventricular mass index in hypertensives with left ventricular hypertrophy on standard ACEI/ARB based drug therapy. MATERIALS AND METHODS: The cohort (n=217) comprised of patients with uncontrolled hypertension (blood pressure>140/90 mm of Hg) and left ventricular hypertrophy (left ventricular mass index>115 and 95 gram/square meter in males and females respectively). The add-on drug in ACEI/ARB therapy was either thiazide diuretics (TD) or calcium channel blockers (CCB). Four sub-cohorts were constituted: mono-therapy - group A (n=70, ACEI/ARB), dual-therapy - group B (n=48, ACEI/ARB+TD) and group C (n=51, ACEI/ ARB+CCB), triple therapy - group D (n=48, ACEI/ ARB+TD+CCB). Left ventricular mass index was determined using echocardiography at baseline and after 24 weeks of therapy. RESULTS: There was no significant difference in baseline clinical or demographic variables between group B and group C. Baseline blood pressure and duration of hypertension was greater in group D compared to group A (P<0.001). The reduction in left ventricular mass index (mean ±SD) in the four groups (A to D) was 16.7±18.7, 21.0±20.8, 20.5±15.5 and 29.1±21.5 g/m2 respectively (D>A, P=0.011, B versus C, P=1.00). The corresponding change in blood pressure (systolic/diastolic) was 18.5±13.6/8.9±11.2, 27.5±19.2/12.2±9.3, 23.4±16.7/ 5.4±10.1, 26.6±19.5/10.7±12.8 mm of Hg respectively (systolic, B>A, P=0.027, D>A, P=0.048) (diastolic, B>C, P=0.013). CONCLUSION: Anti-hypertensive treatment with angiotensin converting enzyme inhibitors/angiotensin receptor blockers-based therapy produced graded regression of left ventricular hypertrophy with monotherapy, dual therapy and triple therapy. In dual therapy, add-on of either thiazide diuretics or calcium channel blockers to angiotensin converting enzyme inhibitors/angiotensin receptor blockers showed equal efficacy in regression of left ventricular hypertrophy independent of blood pressure reduction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


