{"title":"用于药物洗脱支架治疗和随访的冠状动脉造影定量分析的实验室间和实验室内差异。","authors":"Shigenori Ito, Kanako Kinoshita, Akiko Endo, Ryoko Kami, Yuko Kotake, Masato Nakamura","doi":"10.1177/1753944720958982","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To evaluate inter-core laboratory variability of quantitative coronary angiography (QCA) parameters in comparison with intra-core laboratory variability in a randomized controlled trial evaluating drug-eluting stents.</p><p><strong>Methods: </strong>A total of 50 patients with 62 coronary lesions were analyzed by four analysis experts belonging to an Angiographic Core Laboratory (ACL: 1 expert) and a Cardiovascular Imaging Core Laboratory (CICL: 3 experts). QCA was based on the same standard operating procedure, but selections of projection and cine frames were at the discretion of each analyst. Inter- and intra-core laboratory variabilities were evaluated by accuracy, precision, Bland Altman analysis, and coefficient of variation.</p><p><strong>Results: </strong>Pre-MLD (minimal lumen diameter) was significantly smaller in results from ACL than those from all CICL experts. Number of analyzed projections did not affect pre-MLD results. Acute gain was larger in ACL than in CICL2. No significant difference was observed in late loss and loss index between inter-core laboratories. Agreement between core labs in the Bland-Altman analysis for each QCA parameter was as follows (mean difference, 95% limits of agreement): pre-MLD (-0.32, -0.74 to 0.10), stent MLD (0.08, -0.28 to 0.44), acute gain (0.22, -0.44 to 0.88), and late loss (-0.07, -0.69 to 0.55). Agreement between analysts in CICL (mean difference, 95% limits of agreement) was: pre MLD (-0.03, -0.37 to 0.31), stent MLD (0.15, -0.15 to 0.45), acute gain (0.05, -0.45 to 0.55), and late loss (0.04, -0.52 to 0.60). The widest limits of agreement among three analyses were shown in both analyses. Width of limited agreement in the intra-core laboratory analysis tended to be smaller than the inter-core laboratory analysis with these parameters. Coefficient of variation tended to be larger in lesion length (LL), acute gain, late loss, and loss index in inter- and in intra- core laboratory comparisons.</p><p><strong>Conclusion: </strong>Inter-core laboratory QCA variability in late loss and loss index analysis could be similar to intra-core laboratory variability, but more strict alignment between core laboratories would be necessary for initial procedural data analysis.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"14 ","pages":"1753944720958982"},"PeriodicalIF":2.2000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/a2/10.1177_1753944720958982.PMC7534069.pdf","citationCount":"0","resultStr":"{\"title\":\"Inter- and intra-core laboratory variability in the quantitative coronary angiography analysis for drug-eluting stent treatment and follow up.\",\"authors\":\"Shigenori Ito, Kanako Kinoshita, Akiko Endo, Ryoko Kami, Yuko Kotake, Masato Nakamura\",\"doi\":\"10.1177/1753944720958982\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>To evaluate inter-core laboratory variability of quantitative coronary angiography (QCA) parameters in comparison with intra-core laboratory variability in a randomized controlled trial evaluating drug-eluting stents.</p><p><strong>Methods: </strong>A total of 50 patients with 62 coronary lesions were analyzed by four analysis experts belonging to an Angiographic Core Laboratory (ACL: 1 expert) and a Cardiovascular Imaging Core Laboratory (CICL: 3 experts). QCA was based on the same standard operating procedure, but selections of projection and cine frames were at the discretion of each analyst. Inter- and intra-core laboratory variabilities were evaluated by accuracy, precision, Bland Altman analysis, and coefficient of variation.</p><p><strong>Results: </strong>Pre-MLD (minimal lumen diameter) was significantly smaller in results from ACL than those from all CICL experts. Number of analyzed projections did not affect pre-MLD results. Acute gain was larger in ACL than in CICL2. No significant difference was observed in late loss and loss index between inter-core laboratories. Agreement between core labs in the Bland-Altman analysis for each QCA parameter was as follows (mean difference, 95% limits of agreement): pre-MLD (-0.32, -0.74 to 0.10), stent MLD (0.08, -0.28 to 0.44), acute gain (0.22, -0.44 to 0.88), and late loss (-0.07, -0.69 to 0.55). Agreement between analysts in CICL (mean difference, 95% limits of agreement) was: pre MLD (-0.03, -0.37 to 0.31), stent MLD (0.15, -0.15 to 0.45), acute gain (0.05, -0.45 to 0.55), and late loss (0.04, -0.52 to 0.60). The widest limits of agreement among three analyses were shown in both analyses. Width of limited agreement in the intra-core laboratory analysis tended to be smaller than the inter-core laboratory analysis with these parameters. Coefficient of variation tended to be larger in lesion length (LL), acute gain, late loss, and loss index in inter- and in intra- core laboratory comparisons.</p><p><strong>Conclusion: </strong>Inter-core laboratory QCA variability in late loss and loss index analysis could be similar to intra-core laboratory variability, but more strict alignment between core laboratories would be necessary for initial procedural data analysis.</p>\",\"PeriodicalId\":23035,\"journal\":{\"name\":\"Therapeutic Advances in Cardiovascular Disease\",\"volume\":\"14 \",\"pages\":\"1753944720958982\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/a2/10.1177_1753944720958982.PMC7534069.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1753944720958982\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1753944720958982","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Inter- and intra-core laboratory variability in the quantitative coronary angiography analysis for drug-eluting stent treatment and follow up.
Aim: To evaluate inter-core laboratory variability of quantitative coronary angiography (QCA) parameters in comparison with intra-core laboratory variability in a randomized controlled trial evaluating drug-eluting stents.
Methods: A total of 50 patients with 62 coronary lesions were analyzed by four analysis experts belonging to an Angiographic Core Laboratory (ACL: 1 expert) and a Cardiovascular Imaging Core Laboratory (CICL: 3 experts). QCA was based on the same standard operating procedure, but selections of projection and cine frames were at the discretion of each analyst. Inter- and intra-core laboratory variabilities were evaluated by accuracy, precision, Bland Altman analysis, and coefficient of variation.
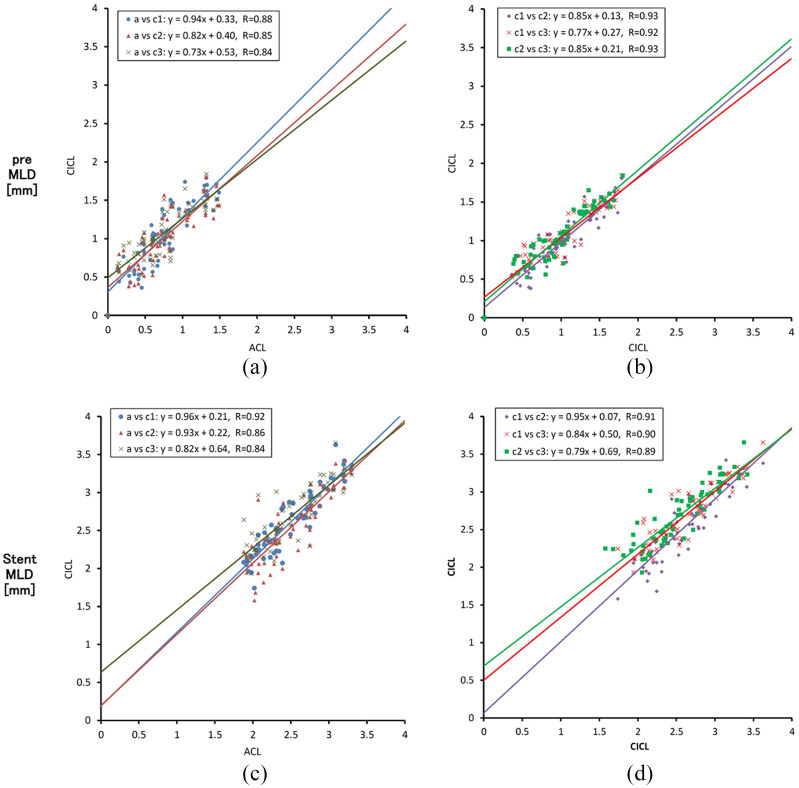
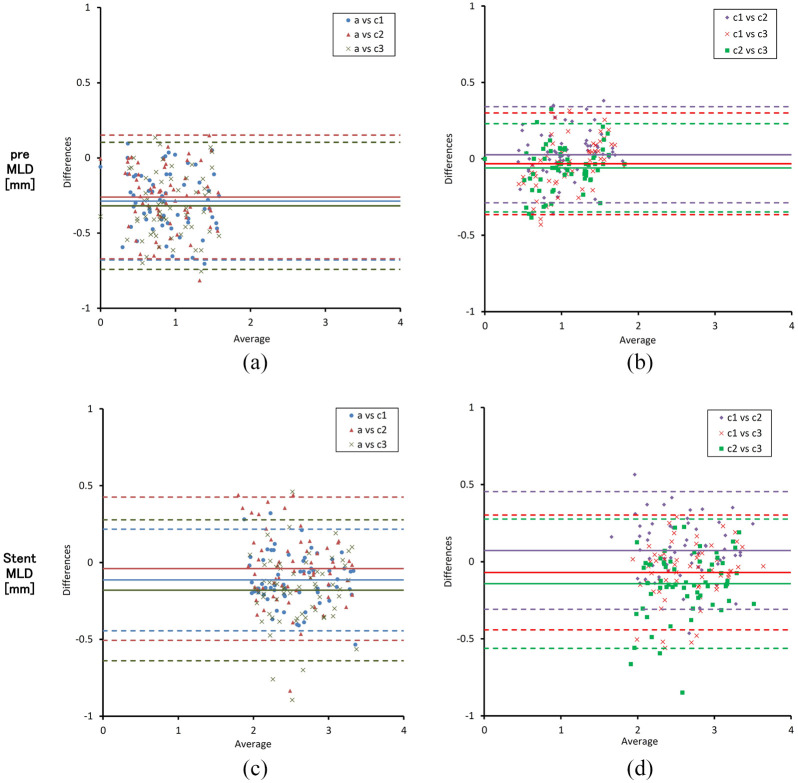
Results: Pre-MLD (minimal lumen diameter) was significantly smaller in results from ACL than those from all CICL experts. Number of analyzed projections did not affect pre-MLD results. Acute gain was larger in ACL than in CICL2. No significant difference was observed in late loss and loss index between inter-core laboratories. Agreement between core labs in the Bland-Altman analysis for each QCA parameter was as follows (mean difference, 95% limits of agreement): pre-MLD (-0.32, -0.74 to 0.10), stent MLD (0.08, -0.28 to 0.44), acute gain (0.22, -0.44 to 0.88), and late loss (-0.07, -0.69 to 0.55). Agreement between analysts in CICL (mean difference, 95% limits of agreement) was: pre MLD (-0.03, -0.37 to 0.31), stent MLD (0.15, -0.15 to 0.45), acute gain (0.05, -0.45 to 0.55), and late loss (0.04, -0.52 to 0.60). The widest limits of agreement among three analyses were shown in both analyses. Width of limited agreement in the intra-core laboratory analysis tended to be smaller than the inter-core laboratory analysis with these parameters. Coefficient of variation tended to be larger in lesion length (LL), acute gain, late loss, and loss index in inter- and in intra- core laboratory comparisons.
Conclusion: Inter-core laboratory QCA variability in late loss and loss index analysis could be similar to intra-core laboratory variability, but more strict alignment between core laboratories would be necessary for initial procedural data analysis.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


