Elizabeth A Cohen, Danielle McKimmy, Anna Cerilli, Sanjay Kulkarni
{"title":"一个药剂师驱动的干预,旨在提高门诊肾移植的用药准确性。","authors":"Elizabeth A Cohen, Danielle McKimmy, Anna Cerilli, Sanjay Kulkarni","doi":"10.2147/DHPS.S264022","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Medication errors are one of the leading causes of complications and readmissions in healthcare and stem directly from inadequate medication lists. In transplantation, medication discrepancies can lead to fluctuating levels of immunosuppression, resulting in rejection, infection, or drug toxicity.</p><p><strong>Methods: </strong>We implemented a pharmacist-driven intervention designed to improve the accuracy of outpatient kidney transplant patients' medication lists in the electronic medical record (EMR). Baseline medication error rates (Phase 1) were collected, and the intervention was a dedicated pharmacist (Phase 2) who performed medication reconciliation with patients. The primary outcome was the percent of patients with inadequate medication reconciliation determined by any one error in medication reconciliation (Phase 1 vs Phase 2). Secondary outcomes included the number of medication errors, of all medications and high-risk medications, identified per patient sample using statistical process control phase analysis.</p><p><strong>Results: </strong>Pharmacist-driven medication reconciliation significantly reduced medication list discrepancies from 95% to 28% (<i>P</i><0.05). There were a total of 398 errors in the control group and 49 errors in the intervention group. In addition, there were 73 high-risk medication discrepancies in the control group and three in the intervention group. The total number of medication errors decreased post-intervention with a marked reduction in the variation of control limits (LCL, UCL: phase 1, -34.3, 113.9; phase 2, -7.1, 15.3) and average number of medication errors per sample (phase 1, 39.8; phase 2, 14.1). For high-risk medications, phase analysis demonstrated a marked reduction in control limit variation between phases (LCL, UCL: phase 1, -10.4, 25.0; phase 2, -0.5, 0.7) and average number of medication errors per sample (phase 1, 7.3; phase 2, 0.1).</p><p><strong>Discussion: </strong>A dedicated pharmacist improved medication list accuracy over conventional practice that utilizes transplant nurses and physicians. Further studies into the cost-effectiveness of this strategy should further justify this approach.</p>","PeriodicalId":11377,"journal":{"name":"Drug, Healthcare and Patient Safety","volume":"12 ","pages":"229-235"},"PeriodicalIF":3.4000,"publicationDate":"2020-11-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/DHPS.S264022","citationCount":"9","resultStr":"{\"title\":\"A Pharmacist-Driven Intervention Designed to Improve Medication Accuracy in the Outpatient Kidney Transplant Setting.\",\"authors\":\"Elizabeth A Cohen, Danielle McKimmy, Anna Cerilli, Sanjay Kulkarni\",\"doi\":\"10.2147/DHPS.S264022\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Medication errors are one of the leading causes of complications and readmissions in healthcare and stem directly from inadequate medication lists. In transplantation, medication discrepancies can lead to fluctuating levels of immunosuppression, resulting in rejection, infection, or drug toxicity.</p><p><strong>Methods: </strong>We implemented a pharmacist-driven intervention designed to improve the accuracy of outpatient kidney transplant patients' medication lists in the electronic medical record (EMR). Baseline medication error rates (Phase 1) were collected, and the intervention was a dedicated pharmacist (Phase 2) who performed medication reconciliation with patients. The primary outcome was the percent of patients with inadequate medication reconciliation determined by any one error in medication reconciliation (Phase 1 vs Phase 2). Secondary outcomes included the number of medication errors, of all medications and high-risk medications, identified per patient sample using statistical process control phase analysis.</p><p><strong>Results: </strong>Pharmacist-driven medication reconciliation significantly reduced medication list discrepancies from 95% to 28% (<i>P</i><0.05). There were a total of 398 errors in the control group and 49 errors in the intervention group. In addition, there were 73 high-risk medication discrepancies in the control group and three in the intervention group. The total number of medication errors decreased post-intervention with a marked reduction in the variation of control limits (LCL, UCL: phase 1, -34.3, 113.9; phase 2, -7.1, 15.3) and average number of medication errors per sample (phase 1, 39.8; phase 2, 14.1). For high-risk medications, phase analysis demonstrated a marked reduction in control limit variation between phases (LCL, UCL: phase 1, -10.4, 25.0; phase 2, -0.5, 0.7) and average number of medication errors per sample (phase 1, 7.3; phase 2, 0.1).</p><p><strong>Discussion: </strong>A dedicated pharmacist improved medication list accuracy over conventional practice that utilizes transplant nurses and physicians. Further studies into the cost-effectiveness of this strategy should further justify this approach.</p>\",\"PeriodicalId\":11377,\"journal\":{\"name\":\"Drug, Healthcare and Patient Safety\",\"volume\":\"12 \",\"pages\":\"229-235\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2020-11-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.2147/DHPS.S264022\",\"citationCount\":\"9\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug, Healthcare and Patient Safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/DHPS.S264022\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug, Healthcare and Patient Safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/DHPS.S264022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
A Pharmacist-Driven Intervention Designed to Improve Medication Accuracy in the Outpatient Kidney Transplant Setting.
Background: Medication errors are one of the leading causes of complications and readmissions in healthcare and stem directly from inadequate medication lists. In transplantation, medication discrepancies can lead to fluctuating levels of immunosuppression, resulting in rejection, infection, or drug toxicity.
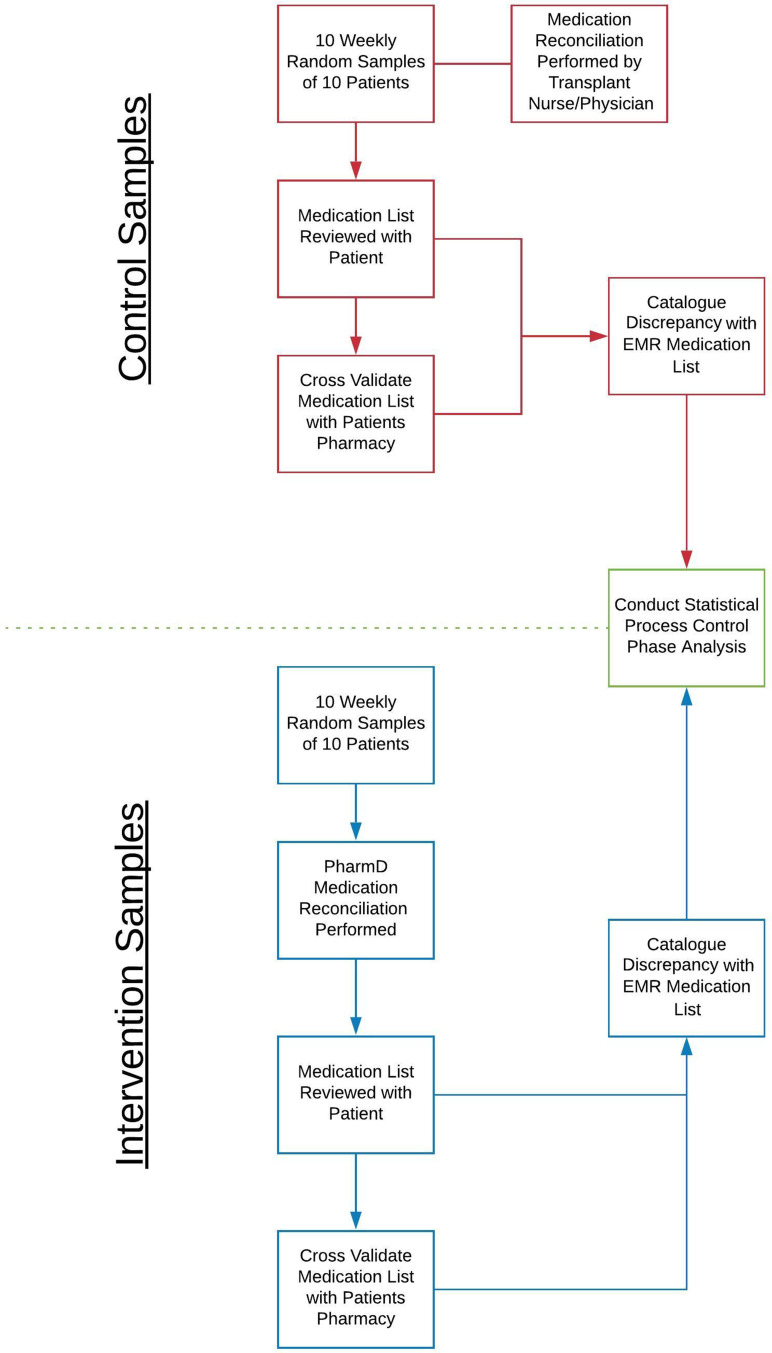
Methods: We implemented a pharmacist-driven intervention designed to improve the accuracy of outpatient kidney transplant patients' medication lists in the electronic medical record (EMR). Baseline medication error rates (Phase 1) were collected, and the intervention was a dedicated pharmacist (Phase 2) who performed medication reconciliation with patients. The primary outcome was the percent of patients with inadequate medication reconciliation determined by any one error in medication reconciliation (Phase 1 vs Phase 2). Secondary outcomes included the number of medication errors, of all medications and high-risk medications, identified per patient sample using statistical process control phase analysis.
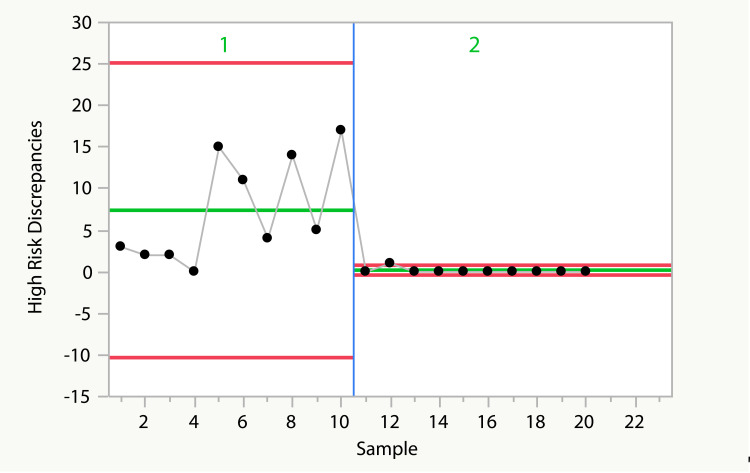
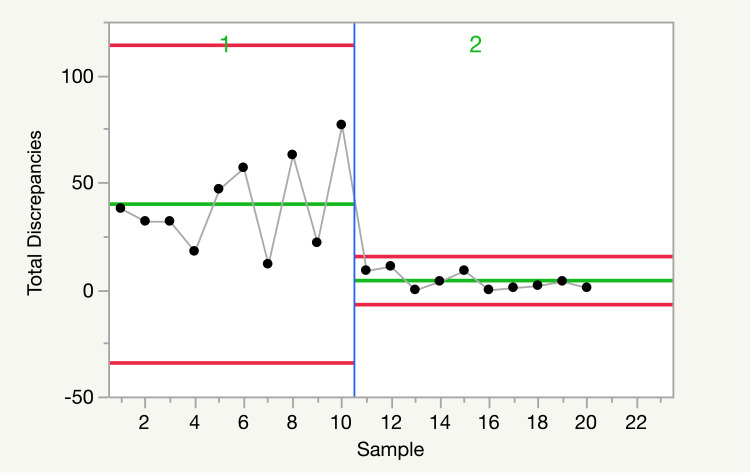
Results: Pharmacist-driven medication reconciliation significantly reduced medication list discrepancies from 95% to 28% (P<0.05). There were a total of 398 errors in the control group and 49 errors in the intervention group. In addition, there were 73 high-risk medication discrepancies in the control group and three in the intervention group. The total number of medication errors decreased post-intervention with a marked reduction in the variation of control limits (LCL, UCL: phase 1, -34.3, 113.9; phase 2, -7.1, 15.3) and average number of medication errors per sample (phase 1, 39.8; phase 2, 14.1). For high-risk medications, phase analysis demonstrated a marked reduction in control limit variation between phases (LCL, UCL: phase 1, -10.4, 25.0; phase 2, -0.5, 0.7) and average number of medication errors per sample (phase 1, 7.3; phase 2, 0.1).
Discussion: A dedicated pharmacist improved medication list accuracy over conventional practice that utilizes transplant nurses and physicians. Further studies into the cost-effectiveness of this strategy should further justify this approach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


