{"title":"胎盘间充质发育不良:超声特征和诊断缺陷。","authors":"Alexandros Psarris, Michail Sindos, Ploutarchos Kourtis, Andreas Pampanos, Panagiotis Antsaklis, Marianna Theodora, Maria Eleni Chondrogianni, Georgios Morphopoulos, Dimitrios Loutradis, Georgios Daskalakis","doi":"10.1055/a-1180-9571","DOIUrl":null,"url":null,"abstract":"<p><p>Placental mesenchymal dysplasia (PMD) is a rare, benign developmental anomaly with a reported prevalence of 0.02% (Arizawa and Nakayama, 2002). It is characterized by placentomegaly with multiple cystic lesions of the stem villi and vascular anomalies (Pawoo and Heller, 2014). Early detection of PMD has been described during routine prenatal ultrasound (Vaisbuch et al., 2009). The sonographic characteristics of PMD include increased placental thickness and multiple cystic areas within the placenta with either an absence of blood flow or with low venous Doppler signals (Vaisbuch et al., 2009). The differential diagnosis of multicystic placental lesions with the presence of a live fetus include partial molar pregnancy, multiple hematomas, chorioangioma Beckwith-Wiedemann syndrome and PMD. Chorioangiomas are well circumscribed masses within the placenta and they are characterized by the presence of a single feeding vessel with the same pulse rate as the umbilical cord (Zalel et al., 2002). Invasive prenatal testing is required for the exclusion of partial molar pregnancy and Beckwith-Wiedemann Syndrome (Vaisbuch et al., 2009). Definitive diagnosis of PMD is based on the pathologic examination of the placenta. Histology reveals aneurysm or dilated blood vessels that may be thrombosed. The stem villi are edematous and enlarged with thick-walled vessels, without trophoblastic proliferation (Pawoo and Heller, 2014). This case report highlights the significance of the early detection of PMD, illustrates the pitfalls in differential diagnosis and provides valuable insights regarding PMD management in a clinical setting.</p>","PeriodicalId":44852,"journal":{"name":"Ultrasound International Open","volume":"6 1","pages":"E2-E3"},"PeriodicalIF":1.6000,"publicationDate":"2020-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/a-1180-9571","citationCount":"3","resultStr":"{\"title\":\"Placental Mesenchymal Dysplasia: Ultrasound Characteristics and Diagnostic Pitfalls.\",\"authors\":\"Alexandros Psarris, Michail Sindos, Ploutarchos Kourtis, Andreas Pampanos, Panagiotis Antsaklis, Marianna Theodora, Maria Eleni Chondrogianni, Georgios Morphopoulos, Dimitrios Loutradis, Georgios Daskalakis\",\"doi\":\"10.1055/a-1180-9571\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Placental mesenchymal dysplasia (PMD) is a rare, benign developmental anomaly with a reported prevalence of 0.02% (Arizawa and Nakayama, 2002). It is characterized by placentomegaly with multiple cystic lesions of the stem villi and vascular anomalies (Pawoo and Heller, 2014). Early detection of PMD has been described during routine prenatal ultrasound (Vaisbuch et al., 2009). The sonographic characteristics of PMD include increased placental thickness and multiple cystic areas within the placenta with either an absence of blood flow or with low venous Doppler signals (Vaisbuch et al., 2009). The differential diagnosis of multicystic placental lesions with the presence of a live fetus include partial molar pregnancy, multiple hematomas, chorioangioma Beckwith-Wiedemann syndrome and PMD. Chorioangiomas are well circumscribed masses within the placenta and they are characterized by the presence of a single feeding vessel with the same pulse rate as the umbilical cord (Zalel et al., 2002). Invasive prenatal testing is required for the exclusion of partial molar pregnancy and Beckwith-Wiedemann Syndrome (Vaisbuch et al., 2009). Definitive diagnosis of PMD is based on the pathologic examination of the placenta. Histology reveals aneurysm or dilated blood vessels that may be thrombosed. The stem villi are edematous and enlarged with thick-walled vessels, without trophoblastic proliferation (Pawoo and Heller, 2014). This case report highlights the significance of the early detection of PMD, illustrates the pitfalls in differential diagnosis and provides valuable insights regarding PMD management in a clinical setting.</p>\",\"PeriodicalId\":44852,\"journal\":{\"name\":\"Ultrasound International Open\",\"volume\":\"6 1\",\"pages\":\"E2-E3\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2020-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1055/a-1180-9571\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound International Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-1180-9571\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/7/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-1180-9571","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/6 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 3
摘要
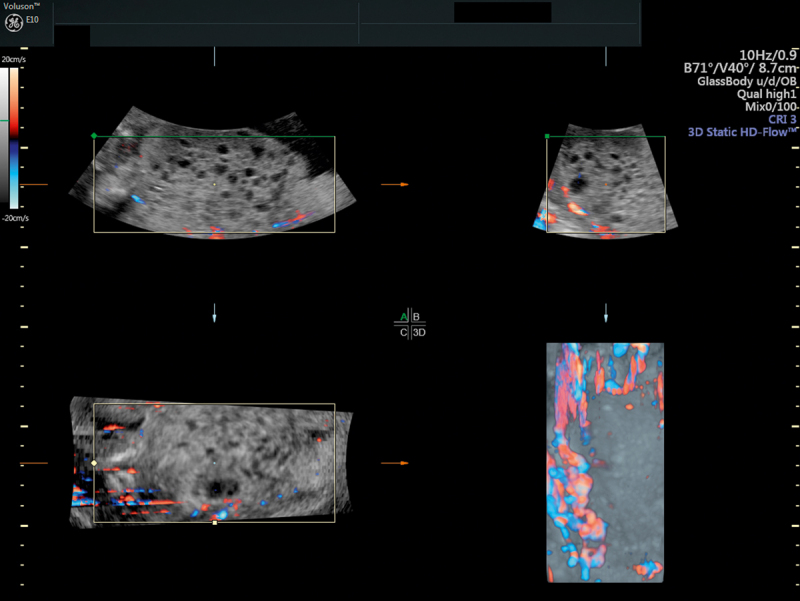
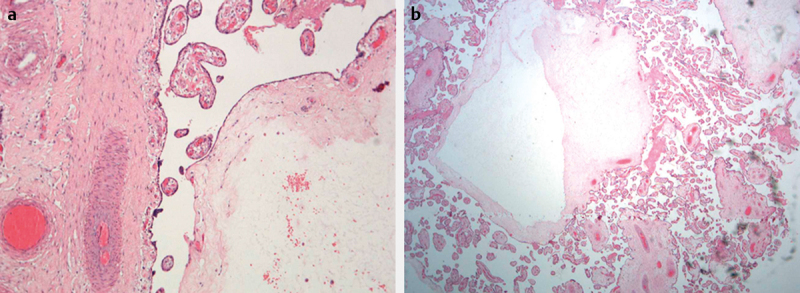
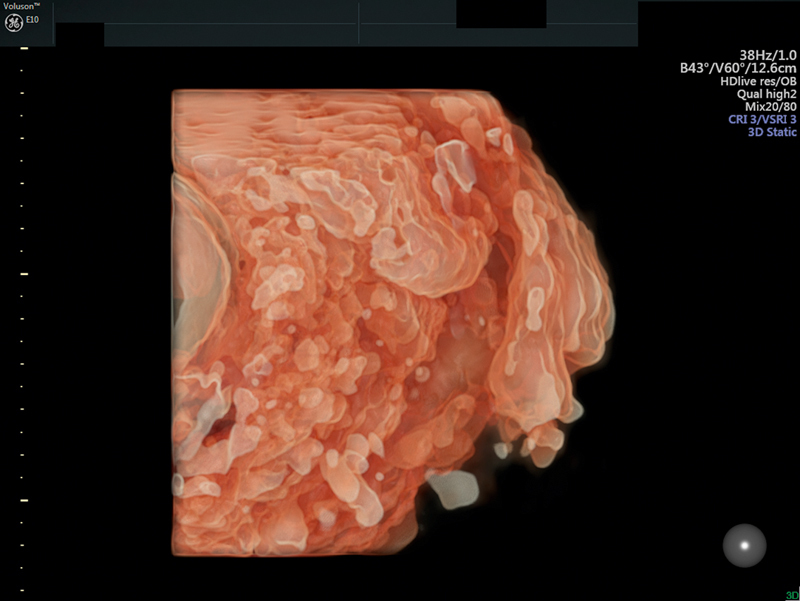
胎盘间充质发育不良(PMD)是一种罕见的良性发育异常,据报道患病率为0.02% (Arizawa and Nakayama, 2002)。其特征是胎盘肿大,并伴有多个茎绒毛囊性病变和血管异常(Pawoo和Heller, 2014)。在常规产前超声检查中已经发现了PMD的早期检测(Vaisbuch et al., 2009)。PMD的超声特征包括胎盘厚度增加和胎盘内多个囊性区域,血流缺乏或静脉多普勒信号低(Vaisbuch et al., 2009)。存在活胎的多囊胎盘病变的鉴别诊断包括部分磨牙妊娠、多发血肿、绒毛膜血管瘤、贝克威氏综合征和经前症候群。绒毛膜血管瘤是胎盘内界限明确的肿块,其特征是存在一条与脐带相同脉搏率的单一喂养血管(Zalel等,2002)。为了排除部分臼齿妊娠和Beckwith-Wiedemann综合征,需要进行侵入性产前检查(Vaisbuch et al., 2009)。明确的诊断PMD是基于病理检查的胎盘。组织学显示动脉瘤或扩张的血管可能形成血栓。茎绒毛水肿、增大,有厚壁血管,没有滋养层增生(Pawoo和Heller, 2014)。本病例报告强调了PMD早期检测的重要性,说明了鉴别诊断的陷阱,并提供了关于临床PMD管理的宝贵见解。
Placental Mesenchymal Dysplasia: Ultrasound Characteristics and Diagnostic Pitfalls.
Placental mesenchymal dysplasia (PMD) is a rare, benign developmental anomaly with a reported prevalence of 0.02% (Arizawa and Nakayama, 2002). It is characterized by placentomegaly with multiple cystic lesions of the stem villi and vascular anomalies (Pawoo and Heller, 2014). Early detection of PMD has been described during routine prenatal ultrasound (Vaisbuch et al., 2009). The sonographic characteristics of PMD include increased placental thickness and multiple cystic areas within the placenta with either an absence of blood flow or with low venous Doppler signals (Vaisbuch et al., 2009). The differential diagnosis of multicystic placental lesions with the presence of a live fetus include partial molar pregnancy, multiple hematomas, chorioangioma Beckwith-Wiedemann syndrome and PMD. Chorioangiomas are well circumscribed masses within the placenta and they are characterized by the presence of a single feeding vessel with the same pulse rate as the umbilical cord (Zalel et al., 2002). Invasive prenatal testing is required for the exclusion of partial molar pregnancy and Beckwith-Wiedemann Syndrome (Vaisbuch et al., 2009). Definitive diagnosis of PMD is based on the pathologic examination of the placenta. Histology reveals aneurysm or dilated blood vessels that may be thrombosed. The stem villi are edematous and enlarged with thick-walled vessels, without trophoblastic proliferation (Pawoo and Heller, 2014). This case report highlights the significance of the early detection of PMD, illustrates the pitfalls in differential diagnosis and provides valuable insights regarding PMD management in a clinical setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


