Jaskaran K Purewal, N F N Sakul, Nikhita R Balabbigari, Alberto Nenninger, Nisha Kotecha
{"title":"一肺战士:肺切除术后综合征并发急性呼吸综合征的通气难题。","authors":"Jaskaran K Purewal, N F N Sakul, Nikhita R Balabbigari, Alberto Nenninger, Nisha Kotecha","doi":"10.1155/2020/5476794","DOIUrl":null,"url":null,"abstract":"<p><p>Postpneumonectomy syndrome involves mediastinal shift causing dynamic airway obstruction via compression of the main bronchus and distal trachea. A few case reports describe the development of ARDS in patients with postpneumonectomy syndrome. Reeb et al. (2017) describe the mortality of postpneumonectomy ARDS anywhere from 33% to 88%. One may encounter difficulty in intubation and ventilation as parameters based on ideal body weight may not apply. Prone positioning ventilation and ECMO have been successfully used in isolated cases. We present such a case and highlight challenges in management. A 70-year-old male Vietnam veteran with remote history of right pneumonectomy thirty years prior presented with fever, cough, and dyspnea. Physical exam was significant for T 36.3°C, BP 162/73, heart rate 145 BPM, RR 22 breaths/minute, ht. 1.72 m, and wt. 78 kg, with transmitted right lung sounds and rhonchi on the left. Labs showed WBC 23.92/nL and procalcitonin 0.84 ng/mL. CXR showed left infiltrate and opacification of right hemithorax with right mediastinal shift. EKG showed atrial fibrillation. He was started on broad spectrum antibiotics for pneumonia, but deteriorated, and was intubated for respiratory distress from ARDS. Vasopressors were initiated for shock. Given the history of pneumonectomy, he was initially ventilated with lower tidal volumes (320 mL). However, incremental changes were made to tidal volumes, and ETT was repositioned several times for hypoxia. Epoprostenol and cisatracurium were also initiated. Positional changes would lead to sudden desaturation; hence, prone positioning ventilation was not done. He was not considered for ECMO due to his pneumonectomy status. Unfortunately, his condition worsened progressively and he expired. The guidelines for ARDS are well established. However, postpneumonectomy patients are unique as seen in our patient. It is unclear whether an endobronchial tube advanced into the left bronchus could have helped difficult airway management resulting from suspected postpneumonectomy syndrome as suggested by CXR. Higher tidal volumes were also unsuccessful in alleviating hypoxia and led to persistently elevated plateau pressures and driving pressures as high as 23, which was inconsistent with our goal of lung protective ventilation. Few case reports describe the successful use of prone positioning ventilation or ECMO in postpneumonectomy patients with ARDS. Although not well studied, low tidal volumes supported with ECMO may have been a favorable strategy for our patient.</p>","PeriodicalId":52364,"journal":{"name":"Case Reports in Pulmonology","volume":"2020 ","pages":"5476794"},"PeriodicalIF":0.0000,"publicationDate":"2020-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/5476794","citationCount":"1","resultStr":"{\"title\":\"One Lung Soldier: A Ventilation Conundrum in a Postpneumonectomy Syndrome Complicated by Acute Respiratory Syndrome.\",\"authors\":\"Jaskaran K Purewal, N F N Sakul, Nikhita R Balabbigari, Alberto Nenninger, Nisha Kotecha\",\"doi\":\"10.1155/2020/5476794\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Postpneumonectomy syndrome involves mediastinal shift causing dynamic airway obstruction via compression of the main bronchus and distal trachea. A few case reports describe the development of ARDS in patients with postpneumonectomy syndrome. Reeb et al. (2017) describe the mortality of postpneumonectomy ARDS anywhere from 33% to 88%. One may encounter difficulty in intubation and ventilation as parameters based on ideal body weight may not apply. Prone positioning ventilation and ECMO have been successfully used in isolated cases. We present such a case and highlight challenges in management. A 70-year-old male Vietnam veteran with remote history of right pneumonectomy thirty years prior presented with fever, cough, and dyspnea. Physical exam was significant for T 36.3°C, BP 162/73, heart rate 145 BPM, RR 22 breaths/minute, ht. 1.72 m, and wt. 78 kg, with transmitted right lung sounds and rhonchi on the left. Labs showed WBC 23.92/nL and procalcitonin 0.84 ng/mL. CXR showed left infiltrate and opacification of right hemithorax with right mediastinal shift. EKG showed atrial fibrillation. He was started on broad spectrum antibiotics for pneumonia, but deteriorated, and was intubated for respiratory distress from ARDS. Vasopressors were initiated for shock. Given the history of pneumonectomy, he was initially ventilated with lower tidal volumes (320 mL). However, incremental changes were made to tidal volumes, and ETT was repositioned several times for hypoxia. Epoprostenol and cisatracurium were also initiated. Positional changes would lead to sudden desaturation; hence, prone positioning ventilation was not done. He was not considered for ECMO due to his pneumonectomy status. Unfortunately, his condition worsened progressively and he expired. The guidelines for ARDS are well established. However, postpneumonectomy patients are unique as seen in our patient. It is unclear whether an endobronchial tube advanced into the left bronchus could have helped difficult airway management resulting from suspected postpneumonectomy syndrome as suggested by CXR. Higher tidal volumes were also unsuccessful in alleviating hypoxia and led to persistently elevated plateau pressures and driving pressures as high as 23, which was inconsistent with our goal of lung protective ventilation. Few case reports describe the successful use of prone positioning ventilation or ECMO in postpneumonectomy patients with ARDS. Although not well studied, low tidal volumes supported with ECMO may have been a favorable strategy for our patient.</p>\",\"PeriodicalId\":52364,\"journal\":{\"name\":\"Case Reports in Pulmonology\",\"volume\":\"2020 \",\"pages\":\"5476794\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-03-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/5476794\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Pulmonology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/5476794\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pulmonology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/5476794","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
摘要
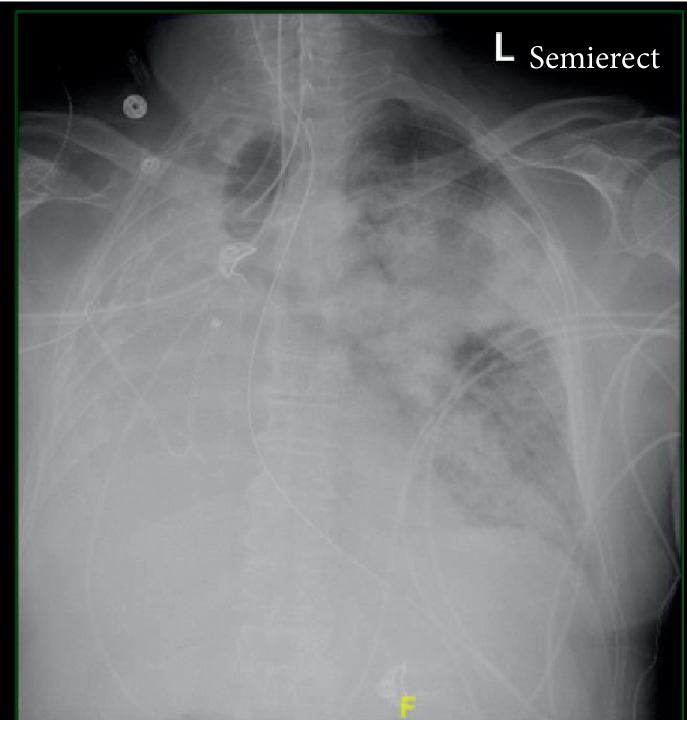
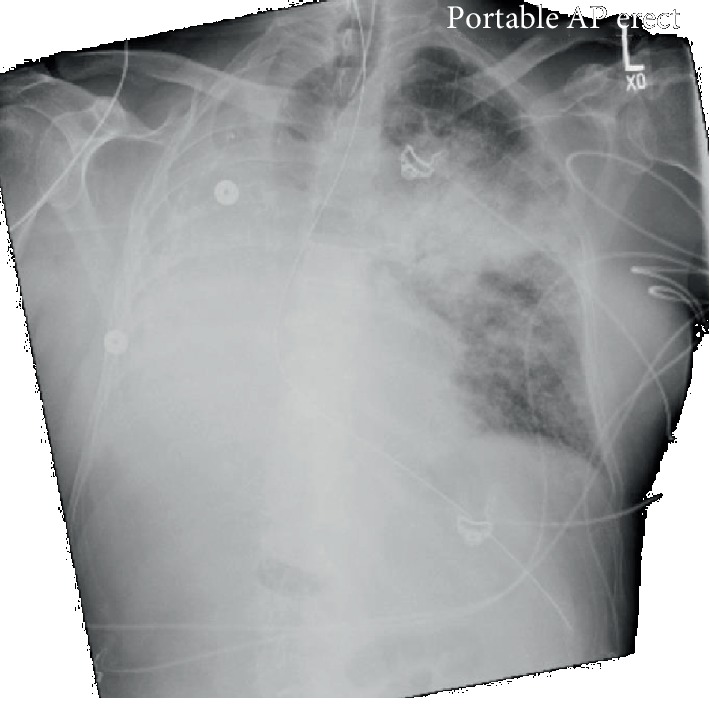
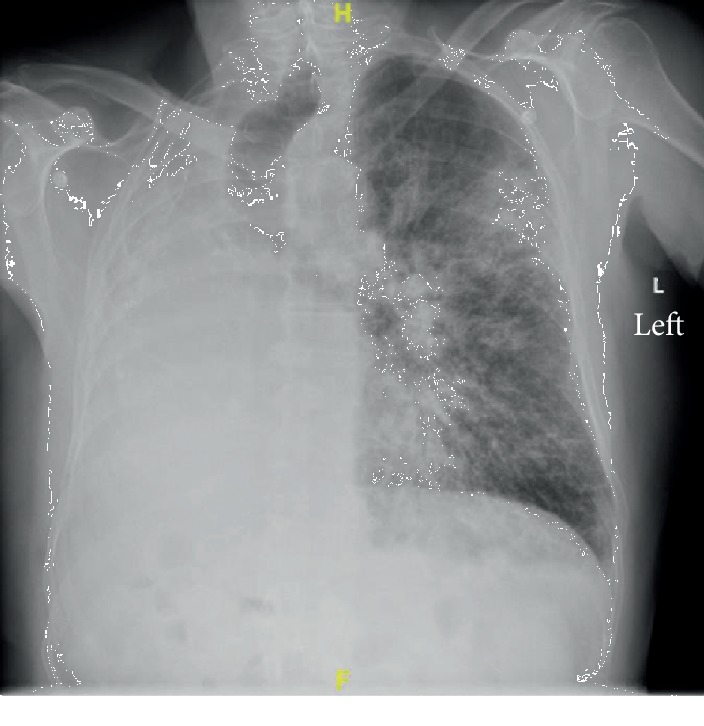
肺切除术后综合征包括纵隔移位,通过压迫主支气管和远端气管引起动态气道阻塞。少数病例报告描述了肺切除术后综合征患者发生ARDS的情况。Reeb等人(2017)描述了肺切除术后ARDS的死亡率从33%到88%不等。患者在插管和通气时可能遇到困难,因为基于理想体重的参数可能不适用。俯卧位通气和ECMO已在个别病例中成功应用。我们提出了这样一个案例,并强调了管理方面的挑战。一位70岁男性越战老兵,30年前有右全肺切除术的病史,目前表现为发烧、咳嗽和呼吸困难。体格检查t36.3°C, BP 162/73,心率145 BPM, RR 22次/分,ht。身高1.72米,体重78公斤,右肺音可传,左肺音可传。实验室WBC 23.92/nL,降钙素原0.84 ng/mL。CXR显示左侧浸润及右侧半胸混浊伴右侧纵隔移位。心电图示心房颤动。他开始使用广谱抗生素治疗肺炎,但病情恶化,并因ARDS呼吸窘迫而插管。开始使用血管加压药治疗休克。考虑到全肺切除史,患者最初采用低潮气量(320 mL)通气。然而,潮汐量发生了渐进式变化,并且由于缺氧,ETT被重新定位了几次。也开始使用丙烯醇和顺阿曲库铵。位置的改变会导致突然的去饱和;因此,未进行俯卧位通气。由于他的全肺切除术状态,没有考虑进行ECMO。不幸的是,他的病情逐渐恶化,最后去世了。急性呼吸窘迫综合征的指导方针已经确立。然而,正如本例患者所见,肺切除术后患者是独特的。目前尚不清楚支气管内管进入左支气管是否有助于气道管理困难,导致疑似肺切除术后综合征,如CXR所示。较高的潮气量也未能缓解缺氧,导致平台压持续升高,驱动压高达23,这与我们肺保护性通气的目标不一致。很少有病例报告描述在肺切除术后ARDS患者中成功使用俯卧位通气或ECMO。虽然没有充分的研究,低潮气量支持ECMO可能是我们的病人有利的策略。
One Lung Soldier: A Ventilation Conundrum in a Postpneumonectomy Syndrome Complicated by Acute Respiratory Syndrome.
Postpneumonectomy syndrome involves mediastinal shift causing dynamic airway obstruction via compression of the main bronchus and distal trachea. A few case reports describe the development of ARDS in patients with postpneumonectomy syndrome. Reeb et al. (2017) describe the mortality of postpneumonectomy ARDS anywhere from 33% to 88%. One may encounter difficulty in intubation and ventilation as parameters based on ideal body weight may not apply. Prone positioning ventilation and ECMO have been successfully used in isolated cases. We present such a case and highlight challenges in management. A 70-year-old male Vietnam veteran with remote history of right pneumonectomy thirty years prior presented with fever, cough, and dyspnea. Physical exam was significant for T 36.3°C, BP 162/73, heart rate 145 BPM, RR 22 breaths/minute, ht. 1.72 m, and wt. 78 kg, with transmitted right lung sounds and rhonchi on the left. Labs showed WBC 23.92/nL and procalcitonin 0.84 ng/mL. CXR showed left infiltrate and opacification of right hemithorax with right mediastinal shift. EKG showed atrial fibrillation. He was started on broad spectrum antibiotics for pneumonia, but deteriorated, and was intubated for respiratory distress from ARDS. Vasopressors were initiated for shock. Given the history of pneumonectomy, he was initially ventilated with lower tidal volumes (320 mL). However, incremental changes were made to tidal volumes, and ETT was repositioned several times for hypoxia. Epoprostenol and cisatracurium were also initiated. Positional changes would lead to sudden desaturation; hence, prone positioning ventilation was not done. He was not considered for ECMO due to his pneumonectomy status. Unfortunately, his condition worsened progressively and he expired. The guidelines for ARDS are well established. However, postpneumonectomy patients are unique as seen in our patient. It is unclear whether an endobronchial tube advanced into the left bronchus could have helped difficult airway management resulting from suspected postpneumonectomy syndrome as suggested by CXR. Higher tidal volumes were also unsuccessful in alleviating hypoxia and led to persistently elevated plateau pressures and driving pressures as high as 23, which was inconsistent with our goal of lung protective ventilation. Few case reports describe the successful use of prone positioning ventilation or ECMO in postpneumonectomy patients with ARDS. Although not well studied, low tidal volumes supported with ECMO may have been a favorable strategy for our patient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


