Oana A Tatucu-Babet, Kate Fetterplace, Kate Lambell, Eliza Miller, Adam M Deane, Emma J Ridley
{"title":"间接量热法指导的能量输送与危重患者临床预后改善相关吗?系统回顾和荟萃分析。","authors":"Oana A Tatucu-Babet, Kate Fetterplace, Kate Lambell, Eliza Miller, Adam M Deane, Emma J Ridley","doi":"10.1177/1178638820903295","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Indirect calorimetry (IC) is recommended to guide energy delivery over predictive equations in critical illness due to its precision. However, the impact of using IC to measure energy expenditure on clinical outcomes is uncertain.</p><p><strong>Objective: </strong>To evaluate whether using IC to measure energy expenditure to inform energy delivery reduced hospital mortality and improved other important outcomes compared to using predictive equations in critically ill adults.</p><p><strong>Methods: </strong>A systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses guideline. Medline, Embase, CINAHL, and the Cochrane Library were searched for studies using IC to guide energy delivery compared to a predictive equation in adult critically ill patients with the primary outcome (hospital mortality) or any of the secondary outcomes reported (including but not limited to hospital and intensive care unit (ICU) length of stay (LOS) and duration mechanical ventilation (MV). Risk of bias within studies was assessed using the Cochrane \"Risk of Bias\" 1 tool. Random-effect meta-analyses were used when heterogeneity between studies existed (I<sup>2</sup> > 50%). Data are reported as median (interquartile range [IQR]), binomial outcomes as odds ratio (OR), 95% confidence interval (CI), and continuous outcomes as mean difference (MD).</p><p><strong>Results: </strong>Of 4060 articles, 4 randomized controlled trials were identified with 396 patients included in analysis. Three studies were considered low risk of bias and 1 as high risk. Two studies reported hospital mortality (n = 130 and 40 participants, respectively). When combined, no association between IC-guided energy delivery and hospital mortality was found (OR = 0.81, 95% CI = [0.25, 2.67], <i>P</i> = 0.73, I<sup>2</sup> = 52). No differences were reported with ICU mortality and hospital LOS between groups, but ICU LOS and duration of MV varied across all studies. According to the meta-analysis, no differences were observed in ICU LOS (MD = 1.39, 95% CI = [-5.01, 7.79], <i>P</i> = 0.67, I<sup>2</sup> = 81%), although the duration of MV was increased when energy delivery was guided by IC (MD = 2.01, 95% CI = [0.45, 3.57], <i>P</i> = 0.01, I<sup>2</sup> = 26%). In all 4 studies, prescribed energy targets were more closely met when energy delivery was informed by IC compared to a predictive equation. Three studies reported the percentage delivered versus the prescribed energy target, with the median (IQR) delta between the IC and predictive equation arms 19% (10%-32%).</p><p><strong>Conclusion: </strong>Limited data exist to assess the impact of using IC to inform energy delivery in comparison to predictive equations on hospital mortality. The association of IC use with other important outcomes, including duration of MV, needs to be further explored before definitive conclusions can be made.</p>","PeriodicalId":19396,"journal":{"name":"Nutrition and Metabolic Insights","volume":"13 ","pages":"1178638820903295"},"PeriodicalIF":2.3000,"publicationDate":"2020-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1178638820903295","citationCount":"16","resultStr":"{\"title\":\"Is Energy Delivery Guided by Indirect Calorimetry Associated With Improved Clinical Outcomes in Critically Ill Patients? A Systematic Review and Meta-analysis.\",\"authors\":\"Oana A Tatucu-Babet, Kate Fetterplace, Kate Lambell, Eliza Miller, Adam M Deane, Emma J Ridley\",\"doi\":\"10.1177/1178638820903295\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Indirect calorimetry (IC) is recommended to guide energy delivery over predictive equations in critical illness due to its precision. However, the impact of using IC to measure energy expenditure on clinical outcomes is uncertain.</p><p><strong>Objective: </strong>To evaluate whether using IC to measure energy expenditure to inform energy delivery reduced hospital mortality and improved other important outcomes compared to using predictive equations in critically ill adults.</p><p><strong>Methods: </strong>A systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses guideline. Medline, Embase, CINAHL, and the Cochrane Library were searched for studies using IC to guide energy delivery compared to a predictive equation in adult critically ill patients with the primary outcome (hospital mortality) or any of the secondary outcomes reported (including but not limited to hospital and intensive care unit (ICU) length of stay (LOS) and duration mechanical ventilation (MV). Risk of bias within studies was assessed using the Cochrane \\\"Risk of Bias\\\" 1 tool. Random-effect meta-analyses were used when heterogeneity between studies existed (I<sup>2</sup> > 50%). Data are reported as median (interquartile range [IQR]), binomial outcomes as odds ratio (OR), 95% confidence interval (CI), and continuous outcomes as mean difference (MD).</p><p><strong>Results: </strong>Of 4060 articles, 4 randomized controlled trials were identified with 396 patients included in analysis. Three studies were considered low risk of bias and 1 as high risk. Two studies reported hospital mortality (n = 130 and 40 participants, respectively). When combined, no association between IC-guided energy delivery and hospital mortality was found (OR = 0.81, 95% CI = [0.25, 2.67], <i>P</i> = 0.73, I<sup>2</sup> = 52). No differences were reported with ICU mortality and hospital LOS between groups, but ICU LOS and duration of MV varied across all studies. According to the meta-analysis, no differences were observed in ICU LOS (MD = 1.39, 95% CI = [-5.01, 7.79], <i>P</i> = 0.67, I<sup>2</sup> = 81%), although the duration of MV was increased when energy delivery was guided by IC (MD = 2.01, 95% CI = [0.45, 3.57], <i>P</i> = 0.01, I<sup>2</sup> = 26%). In all 4 studies, prescribed energy targets were more closely met when energy delivery was informed by IC compared to a predictive equation. Three studies reported the percentage delivered versus the prescribed energy target, with the median (IQR) delta between the IC and predictive equation arms 19% (10%-32%).</p><p><strong>Conclusion: </strong>Limited data exist to assess the impact of using IC to inform energy delivery in comparison to predictive equations on hospital mortality. The association of IC use with other important outcomes, including duration of MV, needs to be further explored before definitive conclusions can be made.</p>\",\"PeriodicalId\":19396,\"journal\":{\"name\":\"Nutrition and Metabolic Insights\",\"volume\":\"13 \",\"pages\":\"1178638820903295\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2020-03-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1178638820903295\",\"citationCount\":\"16\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nutrition and Metabolic Insights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1178638820903295\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"NUTRITION & DIETETICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nutrition and Metabolic Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1178638820903295","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 16
摘要
背景:由于间接量热法(IC)的精确性,它被推荐用于指导危重疾病的能量输送。然而,使用IC测量能量消耗对临床结果的影响是不确定的。目的:评估在危重成人中,与使用预测方程相比,使用IC测量能量消耗以告知能量输送是否降低了医院死亡率并改善了其他重要结果。方法:按照系统评价和荟萃分析指南的首选报告项目进行系统文献综述。Medline, Embase, CINAHL和Cochrane图书馆检索了使用IC指导能量输送的研究,并将其与具有主要结局(住院死亡率)或任何报告的次要结局(包括但不限于医院和重症监护病房(ICU)住院时间(LOS)和机械通气时间(MV)的成年危重患者的预测方程进行了比较。使用Cochrane“偏倚风险”工具评估研究中的偏倚风险。当研究间存在异质性(I2 > 50%)时,采用随机效应荟萃分析。数据以中位数(四分位间距[IQR])报告,以比值比(OR)、95%置信区间(CI)报告二项结果,以平均差(MD)报告连续结果。结果:在4060篇文章中,纳入4项随机对照试验,396例患者纳入分析。3项研究被认为是低风险偏倚,1项研究被认为是高风险偏倚。两项研究报告了住院死亡率(n = 130和40名参与者分别)。综合使用时,ic引导能量输送与住院死亡率无关联(OR = 0.81, 95% CI = [0.25, 2.67], P = 0.73, I2 = 52)。ICU死亡率和住院时间在两组间无差异,但ICU时间和MV持续时间在所有研究中均有差异。meta分析显示,ICU的LOS无差异(MD = 1.39, 95% CI = [-5.01, 7.79], P = 0.67, I2 = 81%),但在IC引导下,MV持续时间增加(MD = 2.01, 95% CI = [0.45, 3.57], P = 0.01, I2 = 26%)。在所有4项研究中,与预测方程相比,当能源交付由IC通知时,规定的能源目标更接近于实现。三项研究报告了与规定能量目标相比的交付百分比,IC和预测方程之间的中位数(IQR) δ为19%(10%-32%)。结论:现有有限的数据来评估使用IC来告知能量输送与预测方程对医院死亡率的影响。在得出明确的结论之前,需要进一步探讨IC使用与其他重要结果(包括MV持续时间)的关系。
Is Energy Delivery Guided by Indirect Calorimetry Associated With Improved Clinical Outcomes in Critically Ill Patients? A Systematic Review and Meta-analysis.
Background: Indirect calorimetry (IC) is recommended to guide energy delivery over predictive equations in critical illness due to its precision. However, the impact of using IC to measure energy expenditure on clinical outcomes is uncertain.
Objective: To evaluate whether using IC to measure energy expenditure to inform energy delivery reduced hospital mortality and improved other important outcomes compared to using predictive equations in critically ill adults.
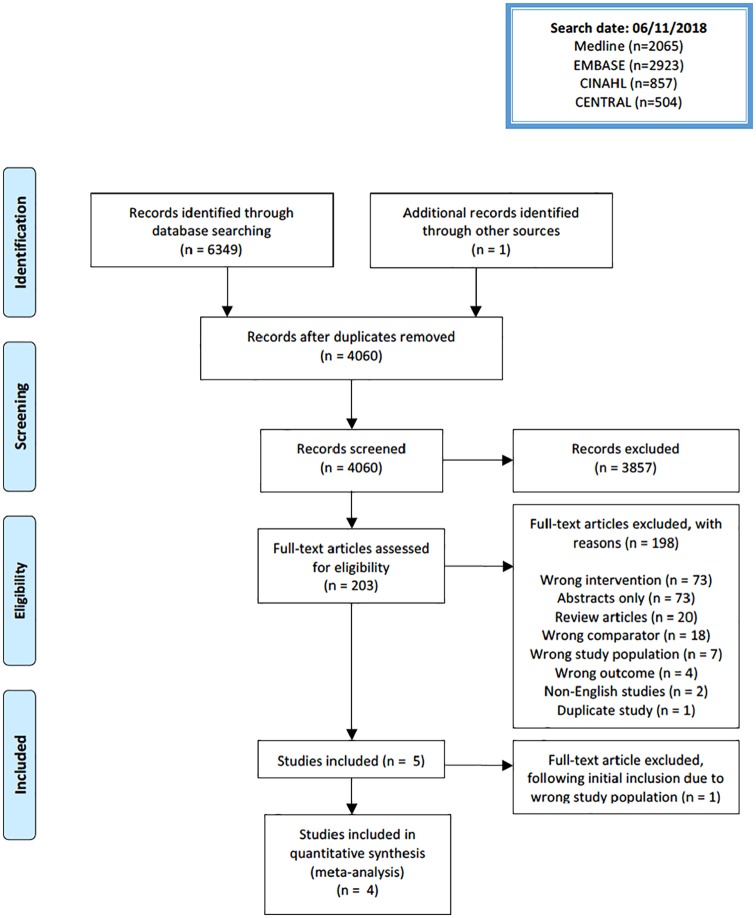
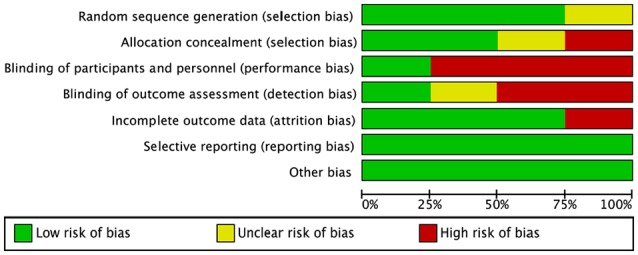
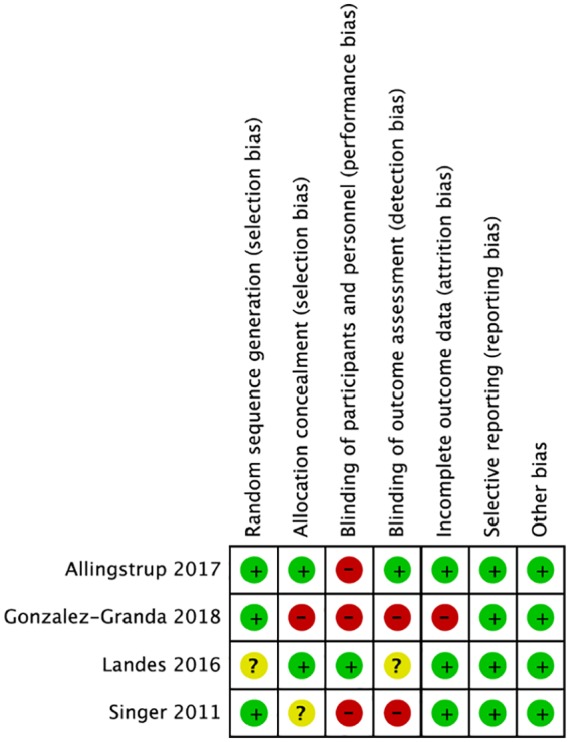
Methods: A systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses guideline. Medline, Embase, CINAHL, and the Cochrane Library were searched for studies using IC to guide energy delivery compared to a predictive equation in adult critically ill patients with the primary outcome (hospital mortality) or any of the secondary outcomes reported (including but not limited to hospital and intensive care unit (ICU) length of stay (LOS) and duration mechanical ventilation (MV). Risk of bias within studies was assessed using the Cochrane "Risk of Bias" 1 tool. Random-effect meta-analyses were used when heterogeneity between studies existed (I2 > 50%). Data are reported as median (interquartile range [IQR]), binomial outcomes as odds ratio (OR), 95% confidence interval (CI), and continuous outcomes as mean difference (MD).
Results: Of 4060 articles, 4 randomized controlled trials were identified with 396 patients included in analysis. Three studies were considered low risk of bias and 1 as high risk. Two studies reported hospital mortality (n = 130 and 40 participants, respectively). When combined, no association between IC-guided energy delivery and hospital mortality was found (OR = 0.81, 95% CI = [0.25, 2.67], P = 0.73, I2 = 52). No differences were reported with ICU mortality and hospital LOS between groups, but ICU LOS and duration of MV varied across all studies. According to the meta-analysis, no differences were observed in ICU LOS (MD = 1.39, 95% CI = [-5.01, 7.79], P = 0.67, I2 = 81%), although the duration of MV was increased when energy delivery was guided by IC (MD = 2.01, 95% CI = [0.45, 3.57], P = 0.01, I2 = 26%). In all 4 studies, prescribed energy targets were more closely met when energy delivery was informed by IC compared to a predictive equation. Three studies reported the percentage delivered versus the prescribed energy target, with the median (IQR) delta between the IC and predictive equation arms 19% (10%-32%).
Conclusion: Limited data exist to assess the impact of using IC to inform energy delivery in comparison to predictive equations on hospital mortality. The association of IC use with other important outcomes, including duration of MV, needs to be further explored before definitive conclusions can be made.
期刊介绍:
Nutrition and Metabolic Insights is a peer-reviewed, open-access online journal focusing on all aspects of nutrition and metabolism. This encompasses nutrition, including the biochemistry of metabolism, exercise and associated physical processes and also includes clinical articles that relate to metabolism, such as obesity, lipidemias and diabetes. It includes research at the molecular, cellular and organismal levels. This journal welcomes new manuscripts for peer review on the following topics: Nutrition, including the biochemistry of metabolism, Exercise and associated physical processes, Clinical articles that relate to metabolism, such as obesity, lipidemias and diabetes, Research at the molecular, cellular and organismal levels, Other areas of interest include gene-nutrient interactions, the effects of hormones, models of metabolic function, macronutrient interactions, outcomes of changes in diet, and pathophysiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


