Emily Verbus, Mustafa Ascha, Barbara Wilkinson, Mary Montague, Jane Morris, Brian M Mercer, Kavita Shah Arora
{"title":"公共保险与产后避孕偏好和提供的关系。","authors":"Emily Verbus, Mustafa Ascha, Barbara Wilkinson, Mary Montague, Jane Morris, Brian M Mercer, Kavita Shah Arora","doi":"10.2147/OAJC.S231196","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prior studies have noted that public insurance status is associated with increased uptake of postpartum contraception whereas others have pointed to public insurance as a barrier to accessing highly effective forms of contraception.</p><p><strong>Objective: </strong>To assess differences in planned method and provision of postpartum contraception according to insurance type.</p><p><strong>Study design: </strong>This is a secondary analysis of a retrospective cohort study examining postpartum women delivered at a single hospital in Cleveland, Ohio from 2012-2014. Contraceptive methods were analyzed according to Tier-based effectiveness as defined by the Centers for Disease Control and Prevention. The primary outcome was postpartum contraception method preference. Additional outcomes included method provision, postpartum visit attendance, and subsequent pregnancy within 365 days of delivery.</p><p><strong>Results: </strong>Of the 8281 patients in the study cohort, 1372 (16.6%) were privately and 6990 (83.4%) were publicly insured. After adjusting for the potentially confounding clinical and demographic factors through propensity score analysis, public insurance was not associated with preference for a Tier 1 versus Tier 2 postpartum contraceptive method (matched adjusted odds ratio [maOR] 0.89, 95% CI 0.69-1.15), but was associated with a preference for Tier 1/2 vs Tier 3/None (maOR 1.41, 95% CI 1.17-1.69). There was no difference between women with private or public insurance in terms of method provision by 90 days after delivery (maOR 0.94, 95% CI 0.75-1.17). Public insurance status was also associated with decreased postpartum visit attendance (maOR 0.54, 95% CI 0.43-0.68) and increased rates of subsequent pregnancy within 365 days of delivery (maOR 1.29, 95% CI 1.05-1.59).</p><p><strong>Conclusion: </strong>Public insurance status does not serve as a barrier to either the preference or provision of effective postpartum contraception. Women desiring highly- or moderately effective methods of contraception should have these methods provided prior to hospital discharge to minimize barriers to method provision.</p>","PeriodicalId":74348,"journal":{"name":"Open access journal of contraception","volume":"10 ","pages":"103-110"},"PeriodicalIF":2.2000,"publicationDate":"2019-12-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b4/a2/oajc-10-103.PMC6927572.pdf","citationCount":"0","resultStr":"{\"title\":\"The Association of Public Insurance with Postpartum Contraception Preference and Provision.\",\"authors\":\"Emily Verbus, Mustafa Ascha, Barbara Wilkinson, Mary Montague, Jane Morris, Brian M Mercer, Kavita Shah Arora\",\"doi\":\"10.2147/OAJC.S231196\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prior studies have noted that public insurance status is associated with increased uptake of postpartum contraception whereas others have pointed to public insurance as a barrier to accessing highly effective forms of contraception.</p><p><strong>Objective: </strong>To assess differences in planned method and provision of postpartum contraception according to insurance type.</p><p><strong>Study design: </strong>This is a secondary analysis of a retrospective cohort study examining postpartum women delivered at a single hospital in Cleveland, Ohio from 2012-2014. Contraceptive methods were analyzed according to Tier-based effectiveness as defined by the Centers for Disease Control and Prevention. The primary outcome was postpartum contraception method preference. Additional outcomes included method provision, postpartum visit attendance, and subsequent pregnancy within 365 days of delivery.</p><p><strong>Results: </strong>Of the 8281 patients in the study cohort, 1372 (16.6%) were privately and 6990 (83.4%) were publicly insured. After adjusting for the potentially confounding clinical and demographic factors through propensity score analysis, public insurance was not associated with preference for a Tier 1 versus Tier 2 postpartum contraceptive method (matched adjusted odds ratio [maOR] 0.89, 95% CI 0.69-1.15), but was associated with a preference for Tier 1/2 vs Tier 3/None (maOR 1.41, 95% CI 1.17-1.69). There was no difference between women with private or public insurance in terms of method provision by 90 days after delivery (maOR 0.94, 95% CI 0.75-1.17). Public insurance status was also associated with decreased postpartum visit attendance (maOR 0.54, 95% CI 0.43-0.68) and increased rates of subsequent pregnancy within 365 days of delivery (maOR 1.29, 95% CI 1.05-1.59).</p><p><strong>Conclusion: </strong>Public insurance status does not serve as a barrier to either the preference or provision of effective postpartum contraception. Women desiring highly- or moderately effective methods of contraception should have these methods provided prior to hospital discharge to minimize barriers to method provision.</p>\",\"PeriodicalId\":74348,\"journal\":{\"name\":\"Open access journal of contraception\",\"volume\":\"10 \",\"pages\":\"103-110\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2019-12-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b4/a2/oajc-10-103.PMC6927572.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open access journal of contraception\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAJC.S231196\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open access journal of contraception","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAJC.S231196","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:先前的研究指出,公共保险状况与产后避孕的增加有关,而其他人则指出公共保险是获得高效避孕形式的障碍。目的:评价不同保险类型在计划避孕方法和提供产后避孕方面的差异。研究设计:这是对2012-2014年在俄亥俄州克利夫兰一家医院分娩的产后妇女进行回顾性队列研究的二次分析。根据疾病控制和预防中心定义的分层有效性来分析避孕方法。主要结局为产后避孕方法偏好。其他结果包括方法提供、产后访问出勤率和分娩365天内的后续妊娠。结果:在研究队列中的8281例患者中,1372例(16.6%)为私人保险,6990例(83.4%)为公共保险。在通过倾向评分分析调整了潜在的混杂临床和人口因素后,公共保险与对一级产后避孕方法和二级产后避孕方法的偏好无关(匹配调整优势比[maOR] 0.89, 95% CI 0.69-1.15),但与对一级1/2对三级/无避孕方法的偏好相关(maOR 1.41, 95% CI 1.17-1.69)。在分娩后90天,私人保险和公共保险的妇女在方法提供方面没有差异(maOR 0.94, 95% CI 0.75-1.17)。公共保险状况也与产后就诊率下降(maOR 0.54, 95% CI 0.43-0.68)和产后365天内妊娠率增加(maOR 1.29, 95% CI 1.05-1.59)相关。结论:公共保险状况不会成为孕妇选择或提供有效产后避孕措施的障碍。希望获得高度或中等有效避孕方法的妇女应在出院前获得这些方法,以尽量减少提供方法的障碍。
The Association of Public Insurance with Postpartum Contraception Preference and Provision.
Background: Prior studies have noted that public insurance status is associated with increased uptake of postpartum contraception whereas others have pointed to public insurance as a barrier to accessing highly effective forms of contraception.
Objective: To assess differences in planned method and provision of postpartum contraception according to insurance type.
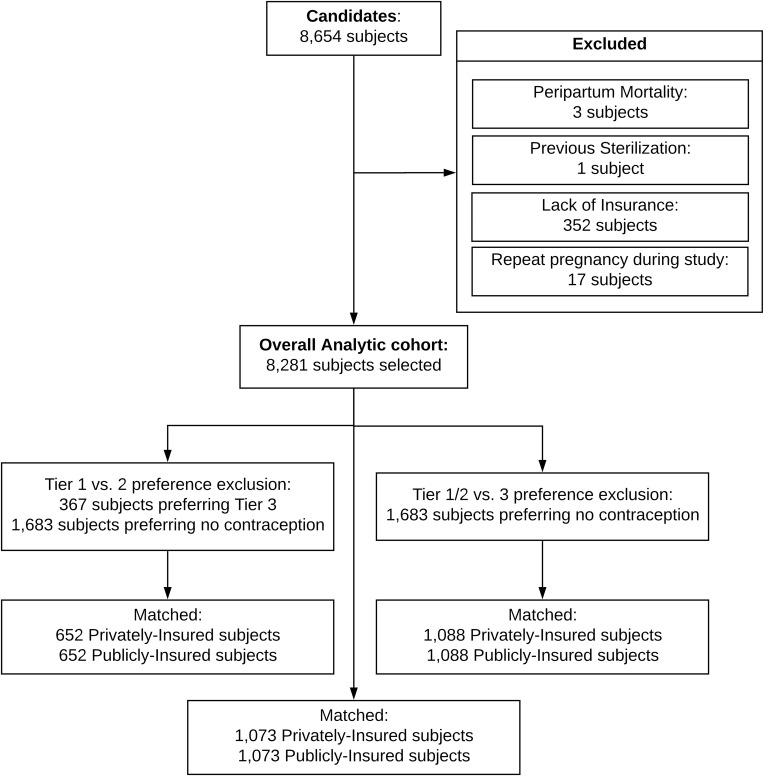
Study design: This is a secondary analysis of a retrospective cohort study examining postpartum women delivered at a single hospital in Cleveland, Ohio from 2012-2014. Contraceptive methods were analyzed according to Tier-based effectiveness as defined by the Centers for Disease Control and Prevention. The primary outcome was postpartum contraception method preference. Additional outcomes included method provision, postpartum visit attendance, and subsequent pregnancy within 365 days of delivery.
Results: Of the 8281 patients in the study cohort, 1372 (16.6%) were privately and 6990 (83.4%) were publicly insured. After adjusting for the potentially confounding clinical and demographic factors through propensity score analysis, public insurance was not associated with preference for a Tier 1 versus Tier 2 postpartum contraceptive method (matched adjusted odds ratio [maOR] 0.89, 95% CI 0.69-1.15), but was associated with a preference for Tier 1/2 vs Tier 3/None (maOR 1.41, 95% CI 1.17-1.69). There was no difference between women with private or public insurance in terms of method provision by 90 days after delivery (maOR 0.94, 95% CI 0.75-1.17). Public insurance status was also associated with decreased postpartum visit attendance (maOR 0.54, 95% CI 0.43-0.68) and increased rates of subsequent pregnancy within 365 days of delivery (maOR 1.29, 95% CI 1.05-1.59).
Conclusion: Public insurance status does not serve as a barrier to either the preference or provision of effective postpartum contraception. Women desiring highly- or moderately effective methods of contraception should have these methods provided prior to hospital discharge to minimize barriers to method provision.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


