Gerrit J Bouma, Martin Barth, Larry E Miller, Sandro Eustacchio, Charlotte Flüh, Richard Bostelmann, Senol Jadik
{"title":"纵向疼痛数据分析的挑战:来自腰椎间盘手术中环闭合随机试验的实践经验。","authors":"Gerrit J Bouma, Martin Barth, Larry E Miller, Sandro Eustacchio, Charlotte Flüh, Richard Bostelmann, Senol Jadik","doi":"10.1155/2019/3498603","DOIUrl":null,"url":null,"abstract":"<p><p><i>Purpose.</i> To analyze leg pain severity data from a randomized controlled trial (RCT) of lumbar disc surgery using integrated approaches that adjust pain scores collected at scheduled follow-up visits for confounding clinical events occurring between visits. <i>Methods.</i> Data were derived from an RCT of a bone-anchored annular closure device (ACD) following lumbar discectomy versus lumbar discectomy alone (Control) in patients with large postsurgical annular defects. Leg pain was recorded on a 0 to 100 scale at 6 weeks, 3 months, 6 months, 1 year, and 2 years of follow-up. Patients with pain reduction ≥20 points relative to baseline were considered responders. Unadjusted analyses utilized pain scores reported at follow-up visits. Since symptomatic reherniation signifies clinical failure of lumbar discectomy, integrated analyses adjusted pain scores following a symptomatic reherniation by baseline observation carried forward for continuous data or classification as nonresponders for categorical data. <i>Results.</i> Among 550 patients (272 ACD, 278 Control), symptomatic reherniation occurred in 10.3% of ACD patients and in 21.9% of controls (<i>p</i> < 0.001) through 2 years. There was no difference in leg pain scores at the 2-year visit between ACD and controls (12 versus 14; <i>p</i> = 0.33) in unadjusted analyses, but statistically significant differences favoring ACD (19 versus 29; <i>p</i> < 0.001) in integrated analyses. Unadjusted nonresponder rates were 6.0% with ACD and 6.7% with controls (<i>p</i> = 0.89), but 15.7% and 27.8% (<i>p</i> = 0.001) in integrated analyses. The probability of nonresponse was 16.4% with ACD and 18.3% with controls (<i>p</i> = 0.51) in unadjusted analysis, and 23.7% and 31.2% (<i>p</i> = 0.04) in integrated analyses. <i>Conclusion</i>. In an RCT of lumbar disc surgery, an integrated analysis of pain severity that adjusted for the confounding effects of clinical failures occurring between follow-up visits resulted in different conclusions compared to an unadjusted analysis of pain scores reported at follow-up visits only.</p>","PeriodicalId":19786,"journal":{"name":"Pain Research and Treatment","volume":"2019 ","pages":"3498603"},"PeriodicalIF":0.0000,"publicationDate":"2019-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2019/3498603","citationCount":"4","resultStr":"{\"title\":\"Challenges in the Analysis of Longitudinal Pain Data: Practical Lessons from a Randomized Trial of Annular Closure in Lumbar Disc Surgery.\",\"authors\":\"Gerrit J Bouma, Martin Barth, Larry E Miller, Sandro Eustacchio, Charlotte Flüh, Richard Bostelmann, Senol Jadik\",\"doi\":\"10.1155/2019/3498603\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><i>Purpose.</i> To analyze leg pain severity data from a randomized controlled trial (RCT) of lumbar disc surgery using integrated approaches that adjust pain scores collected at scheduled follow-up visits for confounding clinical events occurring between visits. <i>Methods.</i> Data were derived from an RCT of a bone-anchored annular closure device (ACD) following lumbar discectomy versus lumbar discectomy alone (Control) in patients with large postsurgical annular defects. Leg pain was recorded on a 0 to 100 scale at 6 weeks, 3 months, 6 months, 1 year, and 2 years of follow-up. Patients with pain reduction ≥20 points relative to baseline were considered responders. Unadjusted analyses utilized pain scores reported at follow-up visits. Since symptomatic reherniation signifies clinical failure of lumbar discectomy, integrated analyses adjusted pain scores following a symptomatic reherniation by baseline observation carried forward for continuous data or classification as nonresponders for categorical data. <i>Results.</i> Among 550 patients (272 ACD, 278 Control), symptomatic reherniation occurred in 10.3% of ACD patients and in 21.9% of controls (<i>p</i> < 0.001) through 2 years. There was no difference in leg pain scores at the 2-year visit between ACD and controls (12 versus 14; <i>p</i> = 0.33) in unadjusted analyses, but statistically significant differences favoring ACD (19 versus 29; <i>p</i> < 0.001) in integrated analyses. Unadjusted nonresponder rates were 6.0% with ACD and 6.7% with controls (<i>p</i> = 0.89), but 15.7% and 27.8% (<i>p</i> = 0.001) in integrated analyses. The probability of nonresponse was 16.4% with ACD and 18.3% with controls (<i>p</i> = 0.51) in unadjusted analysis, and 23.7% and 31.2% (<i>p</i> = 0.04) in integrated analyses. <i>Conclusion</i>. In an RCT of lumbar disc surgery, an integrated analysis of pain severity that adjusted for the confounding effects of clinical failures occurring between follow-up visits resulted in different conclusions compared to an unadjusted analysis of pain scores reported at follow-up visits only.</p>\",\"PeriodicalId\":19786,\"journal\":{\"name\":\"Pain Research and Treatment\",\"volume\":\"2019 \",\"pages\":\"3498603\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-02-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2019/3498603\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pain Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2019/3498603\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/3498603","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Challenges in the Analysis of Longitudinal Pain Data: Practical Lessons from a Randomized Trial of Annular Closure in Lumbar Disc Surgery.
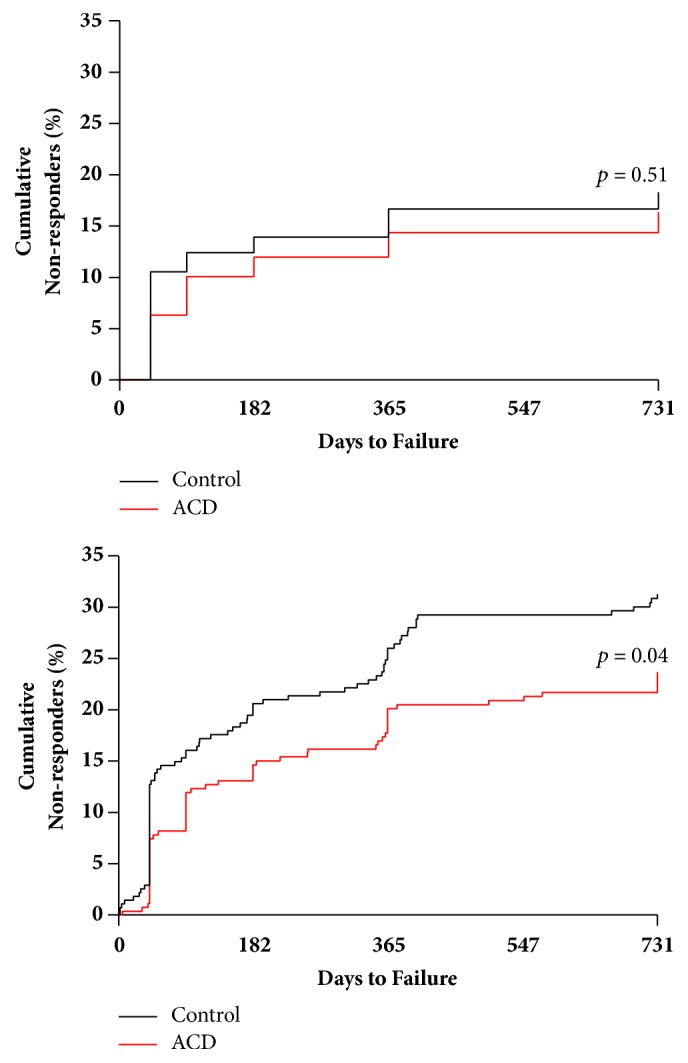
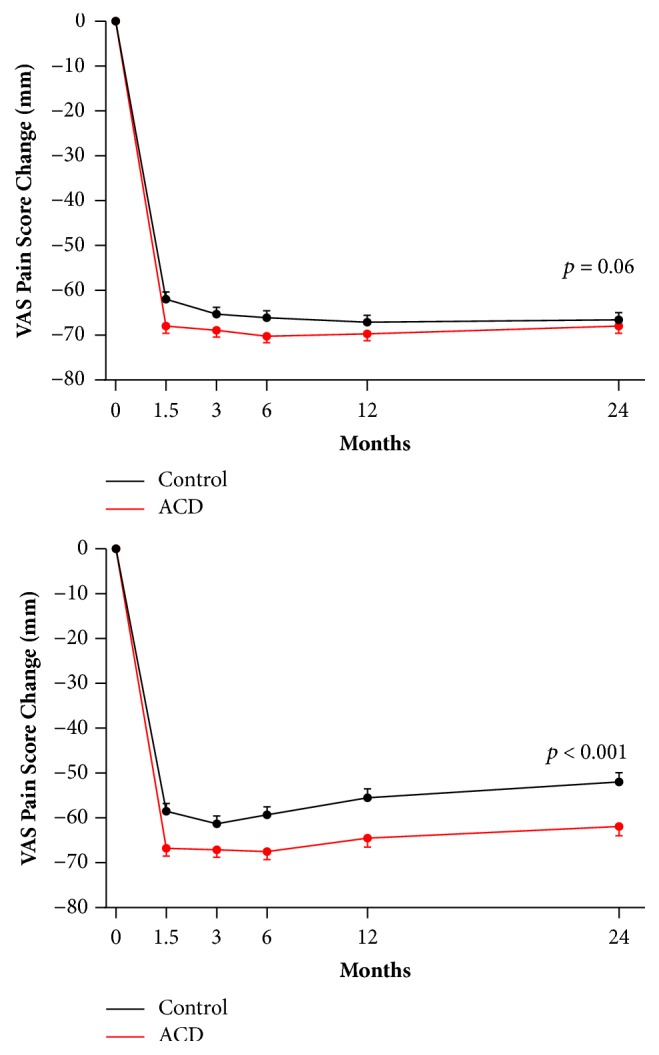
Purpose. To analyze leg pain severity data from a randomized controlled trial (RCT) of lumbar disc surgery using integrated approaches that adjust pain scores collected at scheduled follow-up visits for confounding clinical events occurring between visits. Methods. Data were derived from an RCT of a bone-anchored annular closure device (ACD) following lumbar discectomy versus lumbar discectomy alone (Control) in patients with large postsurgical annular defects. Leg pain was recorded on a 0 to 100 scale at 6 weeks, 3 months, 6 months, 1 year, and 2 years of follow-up. Patients with pain reduction ≥20 points relative to baseline were considered responders. Unadjusted analyses utilized pain scores reported at follow-up visits. Since symptomatic reherniation signifies clinical failure of lumbar discectomy, integrated analyses adjusted pain scores following a symptomatic reherniation by baseline observation carried forward for continuous data or classification as nonresponders for categorical data. Results. Among 550 patients (272 ACD, 278 Control), symptomatic reherniation occurred in 10.3% of ACD patients and in 21.9% of controls (p < 0.001) through 2 years. There was no difference in leg pain scores at the 2-year visit between ACD and controls (12 versus 14; p = 0.33) in unadjusted analyses, but statistically significant differences favoring ACD (19 versus 29; p < 0.001) in integrated analyses. Unadjusted nonresponder rates were 6.0% with ACD and 6.7% with controls (p = 0.89), but 15.7% and 27.8% (p = 0.001) in integrated analyses. The probability of nonresponse was 16.4% with ACD and 18.3% with controls (p = 0.51) in unadjusted analysis, and 23.7% and 31.2% (p = 0.04) in integrated analyses. Conclusion. In an RCT of lumbar disc surgery, an integrated analysis of pain severity that adjusted for the confounding effects of clinical failures occurring between follow-up visits resulted in different conclusions compared to an unadjusted analysis of pain scores reported at follow-up visits only.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


