Shannon M Casillas, Rebecca L Hall, Barbara L Herwaldt
{"title":"环孢子虫病监测-美国,2011-2015。","authors":"Shannon M Casillas, Rebecca L Hall, Barbara L Herwaldt","doi":"10.15585/mmwr.ss6803a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Cyclosporiasis is an intestinal illness caused by the parasite Cyclospora cayetanensis, which is transmissible by ingestion of fecally contaminated food or water. Cyclosporiasis is most common in tropical and subtropical regions of the world. In the United States, foodborne outbreaks of cyclosporiasis have been linked to various types of imported fresh produce (e.g., basil, raspberries, and snow peas). Validated molecular typing tools, which could facilitate detection and investigation of outbreaks, are not yet available for C. cayetanensis.</p><p><strong>Period covered: </strong>2011-2015.</p><p><strong>Description of system: </strong>CDC has been conducting national surveillance for cyclosporiasis since it became a nationally notifiable disease in January 1999. As of 2015, cyclosporiasis was a reportable condition in 42 states, the District of Columbia, and New York City (NYC). Health departments voluntarily notify CDC of cases of cyclosporiasis through the National Notifiable Diseases Surveillance System and submit additional case information using the CDC cyclosporiasis case report form or the Cyclosporiasis National Hypothesis Generating Questionnaire (CNHGQ).</p><p><strong>Results: </strong>For the 2011-2015 surveillance period, CDC was notified by 37 states and NYC of 2,207 cases of cyclosporiasis, including 1,988 confirmed cases (90.1%) and 219 probable cases (9.9%). The annual number of reported cases ranged from 130 in 2012 to 798 in 2013; the annual population-adjusted incidence rate ranged from 0.05 cases per 100,000 persons in 2012 to 0.29 in 2013. A total of 415 patients (18.8%) had a documented history of international travel during the 14 days before illness onset, 1,384 (62.7%) did not have a history of international travel, and 408 (18.5%) had an unknown travel history. Among the 1,359 domestically acquired cases with available information about illness onset, 1,263 (92.9%) occurred among persons who became ill during May-August. During 2011-2015, a total of 10 outbreaks of cyclosporiasis associated with 438 reported cases were investigated; a median of 21 cases were reported per outbreak (range: eight to 162). A food vehicle of infection (i.e., a food item or ingredient thereof) was identified (or suspected) for at least five of the 10 outbreaks; the food vehicles included a berry salad (one outbreak), cilantro imported from Mexico (at least three outbreaks), and a prepackaged salad mix from Mexico (one outbreak).</p><p><strong>Interpretation: </strong>Cyclosporiasis continues to be a U.S. public health concern, with seasonal increases in reported cases during spring and summer months. The majority of cases reported for this 5-year surveillance period occurred among persons without a history of international travel who became ill during May-August. Many of the seemingly sporadic domestically acquired cases might have been associated with identified or unidentified outbreaks; however, those potential associations were not detected using the available epidemiologic information. Prevention of cases and outbreaks of cyclosporiasis in the United States depends on outbreak detection and investigation, including identification of food vehicles of infection and their sources, which could be facilitated by the availability of validated molecular typing tools.</p><p><strong>Public health action: </strong>Surveillance for cases of cyclosporiasis and efforts to develop and validate molecular typing tools should remain U.S. public health priorities. During periods and seasons when increased numbers of domestically acquired cases are reported, the CNHGQ should be used to facilitate outbreak detection and hypothesis generation. Travelers to areas of known endemicity (e.g., in the tropics and subtropics) should follow food and water precautions similar to those for other enteric pathogens but should be advised that use of routine chemical disinfection or sanitizing methods is unlikely to kill C. cayetanensis. Health care providers should consider the possibility of Cyclospora infection in persons with persistent or remitting-relapsing diarrheal illness, especially for persons with a history of travel to areas of known endemicity or with symptom onset during spring or summer. If indicated, laboratory testing for Cyclospora should be explicitly requested because such testing is not typically part of routine examinations for ova and parasites and is not included in all gastrointestinal polymerase chain reaction panels. Newly identified cases of cyclosporiasis should be promptly reported to state or local public health authorities, who are encouraged to notify CDC of the cases.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"68 3","pages":"1-16"},"PeriodicalIF":37.3000,"publicationDate":"2019-04-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6476303/pdf/","citationCount":"13","resultStr":"{\"title\":\"Cyclosporiasis Surveillance - United States, 2011-2015.\",\"authors\":\"Shannon M Casillas, Rebecca L Hall, Barbara L Herwaldt\",\"doi\":\"10.15585/mmwr.ss6803a1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Problem/condition: </strong>Cyclosporiasis is an intestinal illness caused by the parasite Cyclospora cayetanensis, which is transmissible by ingestion of fecally contaminated food or water. Cyclosporiasis is most common in tropical and subtropical regions of the world. In the United States, foodborne outbreaks of cyclosporiasis have been linked to various types of imported fresh produce (e.g., basil, raspberries, and snow peas). Validated molecular typing tools, which could facilitate detection and investigation of outbreaks, are not yet available for C. cayetanensis.</p><p><strong>Period covered: </strong>2011-2015.</p><p><strong>Description of system: </strong>CDC has been conducting national surveillance for cyclosporiasis since it became a nationally notifiable disease in January 1999. As of 2015, cyclosporiasis was a reportable condition in 42 states, the District of Columbia, and New York City (NYC). Health departments voluntarily notify CDC of cases of cyclosporiasis through the National Notifiable Diseases Surveillance System and submit additional case information using the CDC cyclosporiasis case report form or the Cyclosporiasis National Hypothesis Generating Questionnaire (CNHGQ).</p><p><strong>Results: </strong>For the 2011-2015 surveillance period, CDC was notified by 37 states and NYC of 2,207 cases of cyclosporiasis, including 1,988 confirmed cases (90.1%) and 219 probable cases (9.9%). The annual number of reported cases ranged from 130 in 2012 to 798 in 2013; the annual population-adjusted incidence rate ranged from 0.05 cases per 100,000 persons in 2012 to 0.29 in 2013. A total of 415 patients (18.8%) had a documented history of international travel during the 14 days before illness onset, 1,384 (62.7%) did not have a history of international travel, and 408 (18.5%) had an unknown travel history. Among the 1,359 domestically acquired cases with available information about illness onset, 1,263 (92.9%) occurred among persons who became ill during May-August. During 2011-2015, a total of 10 outbreaks of cyclosporiasis associated with 438 reported cases were investigated; a median of 21 cases were reported per outbreak (range: eight to 162). A food vehicle of infection (i.e., a food item or ingredient thereof) was identified (or suspected) for at least five of the 10 outbreaks; the food vehicles included a berry salad (one outbreak), cilantro imported from Mexico (at least three outbreaks), and a prepackaged salad mix from Mexico (one outbreak).</p><p><strong>Interpretation: </strong>Cyclosporiasis continues to be a U.S. public health concern, with seasonal increases in reported cases during spring and summer months. The majority of cases reported for this 5-year surveillance period occurred among persons without a history of international travel who became ill during May-August. Many of the seemingly sporadic domestically acquired cases might have been associated with identified or unidentified outbreaks; however, those potential associations were not detected using the available epidemiologic information. Prevention of cases and outbreaks of cyclosporiasis in the United States depends on outbreak detection and investigation, including identification of food vehicles of infection and their sources, which could be facilitated by the availability of validated molecular typing tools.</p><p><strong>Public health action: </strong>Surveillance for cases of cyclosporiasis and efforts to develop and validate molecular typing tools should remain U.S. public health priorities. During periods and seasons when increased numbers of domestically acquired cases are reported, the CNHGQ should be used to facilitate outbreak detection and hypothesis generation. Travelers to areas of known endemicity (e.g., in the tropics and subtropics) should follow food and water precautions similar to those for other enteric pathogens but should be advised that use of routine chemical disinfection or sanitizing methods is unlikely to kill C. cayetanensis. Health care providers should consider the possibility of Cyclospora infection in persons with persistent or remitting-relapsing diarrheal illness, especially for persons with a history of travel to areas of known endemicity or with symptom onset during spring or summer. If indicated, laboratory testing for Cyclospora should be explicitly requested because such testing is not typically part of routine examinations for ova and parasites and is not included in all gastrointestinal polymerase chain reaction panels. Newly identified cases of cyclosporiasis should be promptly reported to state or local public health authorities, who are encouraged to notify CDC of the cases.</p>\",\"PeriodicalId\":48549,\"journal\":{\"name\":\"Mmwr Surveillance Summaries\",\"volume\":\"68 3\",\"pages\":\"1-16\"},\"PeriodicalIF\":37.3000,\"publicationDate\":\"2019-04-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6476303/pdf/\",\"citationCount\":\"13\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Mmwr Surveillance Summaries\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.15585/mmwr.ss6803a1\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss6803a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Cyclosporiasis Surveillance - United States, 2011-2015.
Problem/condition: Cyclosporiasis is an intestinal illness caused by the parasite Cyclospora cayetanensis, which is transmissible by ingestion of fecally contaminated food or water. Cyclosporiasis is most common in tropical and subtropical regions of the world. In the United States, foodborne outbreaks of cyclosporiasis have been linked to various types of imported fresh produce (e.g., basil, raspberries, and snow peas). Validated molecular typing tools, which could facilitate detection and investigation of outbreaks, are not yet available for C. cayetanensis.
Period covered: 2011-2015.
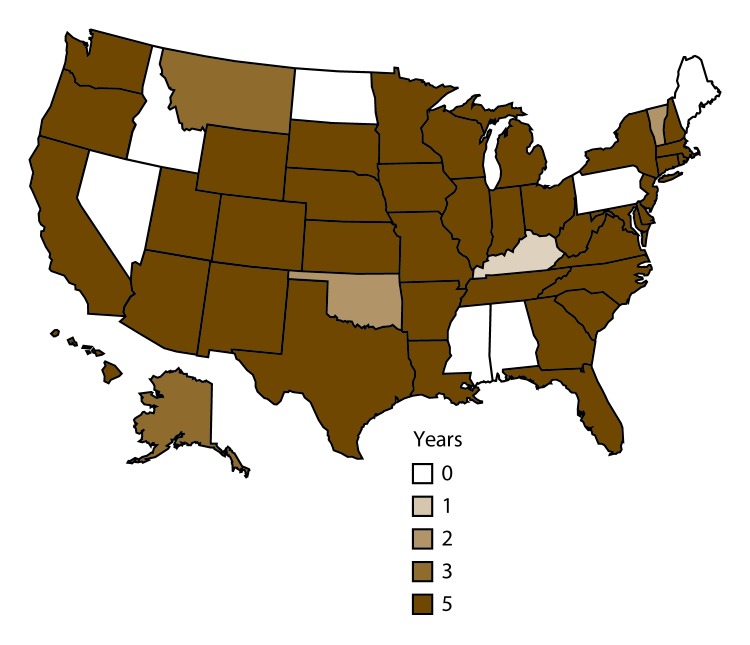
Description of system: CDC has been conducting national surveillance for cyclosporiasis since it became a nationally notifiable disease in January 1999. As of 2015, cyclosporiasis was a reportable condition in 42 states, the District of Columbia, and New York City (NYC). Health departments voluntarily notify CDC of cases of cyclosporiasis through the National Notifiable Diseases Surveillance System and submit additional case information using the CDC cyclosporiasis case report form or the Cyclosporiasis National Hypothesis Generating Questionnaire (CNHGQ).
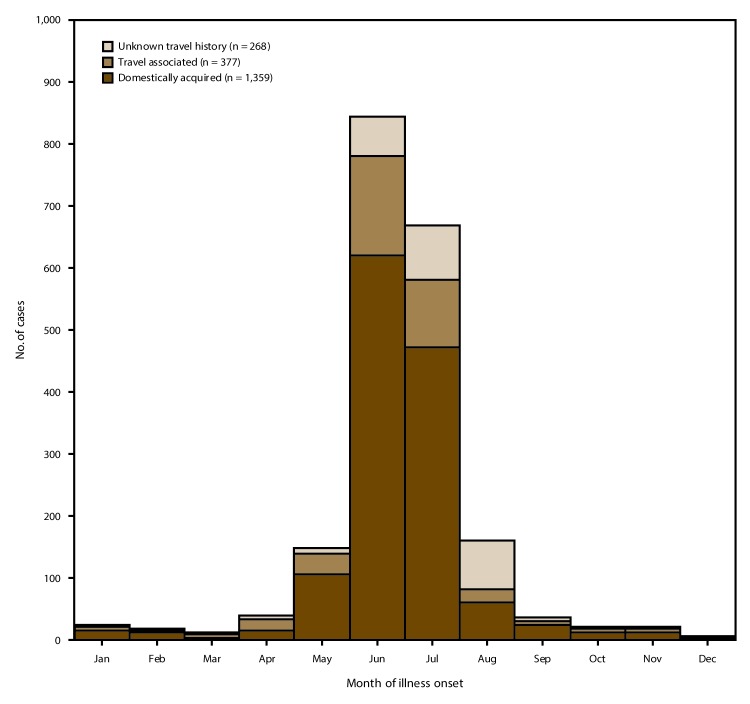
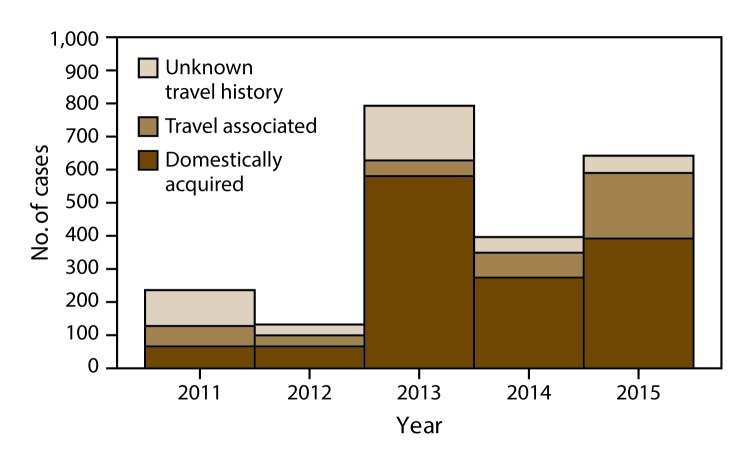
Results: For the 2011-2015 surveillance period, CDC was notified by 37 states and NYC of 2,207 cases of cyclosporiasis, including 1,988 confirmed cases (90.1%) and 219 probable cases (9.9%). The annual number of reported cases ranged from 130 in 2012 to 798 in 2013; the annual population-adjusted incidence rate ranged from 0.05 cases per 100,000 persons in 2012 to 0.29 in 2013. A total of 415 patients (18.8%) had a documented history of international travel during the 14 days before illness onset, 1,384 (62.7%) did not have a history of international travel, and 408 (18.5%) had an unknown travel history. Among the 1,359 domestically acquired cases with available information about illness onset, 1,263 (92.9%) occurred among persons who became ill during May-August. During 2011-2015, a total of 10 outbreaks of cyclosporiasis associated with 438 reported cases were investigated; a median of 21 cases were reported per outbreak (range: eight to 162). A food vehicle of infection (i.e., a food item or ingredient thereof) was identified (or suspected) for at least five of the 10 outbreaks; the food vehicles included a berry salad (one outbreak), cilantro imported from Mexico (at least three outbreaks), and a prepackaged salad mix from Mexico (one outbreak).
Interpretation: Cyclosporiasis continues to be a U.S. public health concern, with seasonal increases in reported cases during spring and summer months. The majority of cases reported for this 5-year surveillance period occurred among persons without a history of international travel who became ill during May-August. Many of the seemingly sporadic domestically acquired cases might have been associated with identified or unidentified outbreaks; however, those potential associations were not detected using the available epidemiologic information. Prevention of cases and outbreaks of cyclosporiasis in the United States depends on outbreak detection and investigation, including identification of food vehicles of infection and their sources, which could be facilitated by the availability of validated molecular typing tools.
Public health action: Surveillance for cases of cyclosporiasis and efforts to develop and validate molecular typing tools should remain U.S. public health priorities. During periods and seasons when increased numbers of domestically acquired cases are reported, the CNHGQ should be used to facilitate outbreak detection and hypothesis generation. Travelers to areas of known endemicity (e.g., in the tropics and subtropics) should follow food and water precautions similar to those for other enteric pathogens but should be advised that use of routine chemical disinfection or sanitizing methods is unlikely to kill C. cayetanensis. Health care providers should consider the possibility of Cyclospora infection in persons with persistent or remitting-relapsing diarrheal illness, especially for persons with a history of travel to areas of known endemicity or with symptom onset during spring or summer. If indicated, laboratory testing for Cyclospora should be explicitly requested because such testing is not typically part of routine examinations for ova and parasites and is not included in all gastrointestinal polymerase chain reaction panels. Newly identified cases of cyclosporiasis should be promptly reported to state or local public health authorities, who are encouraged to notify CDC of the cases.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


