Marcos Edgar Fernández-Cuadros, Gabriela Goizueta-San-Martin, Blanca Varas-de-Dios, Luz Otilia Casique-Bocanegra, Pablo Manrique-de-Lara-Cadiñanos, María Jesus Albaladejo-Florin, Ruben Algarra-López, Olga Susana Pérez-Moro
{"title":"秋水仙碱诱导横纹肌溶解:临床、生化和神经生理特征及文献综述。","authors":"Marcos Edgar Fernández-Cuadros, Gabriela Goizueta-San-Martin, Blanca Varas-de-Dios, Luz Otilia Casique-Bocanegra, Pablo Manrique-de-Lara-Cadiñanos, María Jesus Albaladejo-Florin, Ruben Algarra-López, Olga Susana Pérez-Moro","doi":"10.1177/1179544119849883","DOIUrl":null,"url":null,"abstract":"<p><p>We report the case of a 46-years-old man with long-term asymptomatic hyperuricemia who started taking colchicine (0.5 mg/day) and allopurinol (100 mg/d) for normalization of biochemical values. After the third week of starting treatment, acute weakness was present; and by the fifth week, profound weakness in lower extremities and tenderness and cramps on thighs and calves with inability to climb stairs were also observed. Biochemical evaluation showed elevated muscle enzymes (creatinine kinase [CK] raised to five-folds its normal value) and electromyographic features were consistent with myopathy (at rest, fibrillations, positive sharp waves, high-frequency myotonic discharges; motor unit action potentials [MUAPs] of small amplitude, small duration, increased polyphasic Index and occasional satellite potentials; at maximal effort, interferential recruitment pattern with reduced amplitudes were observed). Normal motor and sensitive nerve conduction studies and normal late <i>F</i>-responses and <i>H</i>-reflex discarded neuropathy. Rapid improvement in muscle strength and prompt resolution of abnormal elevated muscle enzymes was observed after withdrawal of both medications. Colchicine is associated with some cases of myotoxicity but very small cases of colchicine-induced rhabdomyolysis are reported on the literature. Colchicine-induced rhabdomyolysis is related to the concomitant use of drugs (statins, steroids, erythromycin, and cyclosporine), renal, and/or hepatic impairment. To the best of our knowledge, this is an uncommon presentation of a case of colchicine-induced rhabdomyolysis reported in a patient without renal or hepatic dysfunction. Therefore, patients receiving colchicine even in the absence of renal insufficiency should be monitored for the development of myopathy and more rarely to rhabdomyolysis.</p>","PeriodicalId":10443,"journal":{"name":"Clinical Medicine Insights. Arthritis and Musculoskeletal Disorders","volume":"12 ","pages":"1179544119849883"},"PeriodicalIF":1.9000,"publicationDate":"2019-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179544119849883","citationCount":"13","resultStr":"{\"title\":\"Colchicine-Induced Rhabdomyolysis: Clinical, Biochemical, and Neurophysiological Features and Review of the Literature.\",\"authors\":\"Marcos Edgar Fernández-Cuadros, Gabriela Goizueta-San-Martin, Blanca Varas-de-Dios, Luz Otilia Casique-Bocanegra, Pablo Manrique-de-Lara-Cadiñanos, María Jesus Albaladejo-Florin, Ruben Algarra-López, Olga Susana Pérez-Moro\",\"doi\":\"10.1177/1179544119849883\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report the case of a 46-years-old man with long-term asymptomatic hyperuricemia who started taking colchicine (0.5 mg/day) and allopurinol (100 mg/d) for normalization of biochemical values. After the third week of starting treatment, acute weakness was present; and by the fifth week, profound weakness in lower extremities and tenderness and cramps on thighs and calves with inability to climb stairs were also observed. Biochemical evaluation showed elevated muscle enzymes (creatinine kinase [CK] raised to five-folds its normal value) and electromyographic features were consistent with myopathy (at rest, fibrillations, positive sharp waves, high-frequency myotonic discharges; motor unit action potentials [MUAPs] of small amplitude, small duration, increased polyphasic Index and occasional satellite potentials; at maximal effort, interferential recruitment pattern with reduced amplitudes were observed). Normal motor and sensitive nerve conduction studies and normal late <i>F</i>-responses and <i>H</i>-reflex discarded neuropathy. Rapid improvement in muscle strength and prompt resolution of abnormal elevated muscle enzymes was observed after withdrawal of both medications. Colchicine is associated with some cases of myotoxicity but very small cases of colchicine-induced rhabdomyolysis are reported on the literature. Colchicine-induced rhabdomyolysis is related to the concomitant use of drugs (statins, steroids, erythromycin, and cyclosporine), renal, and/or hepatic impairment. To the best of our knowledge, this is an uncommon presentation of a case of colchicine-induced rhabdomyolysis reported in a patient without renal or hepatic dysfunction. Therefore, patients receiving colchicine even in the absence of renal insufficiency should be monitored for the development of myopathy and more rarely to rhabdomyolysis.</p>\",\"PeriodicalId\":10443,\"journal\":{\"name\":\"Clinical Medicine Insights. Arthritis and Musculoskeletal Disorders\",\"volume\":\"12 \",\"pages\":\"1179544119849883\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2019-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179544119849883\",\"citationCount\":\"13\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Arthritis and Musculoskeletal Disorders\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179544119849883\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Arthritis and Musculoskeletal Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179544119849883","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Colchicine-Induced Rhabdomyolysis: Clinical, Biochemical, and Neurophysiological Features and Review of the Literature.
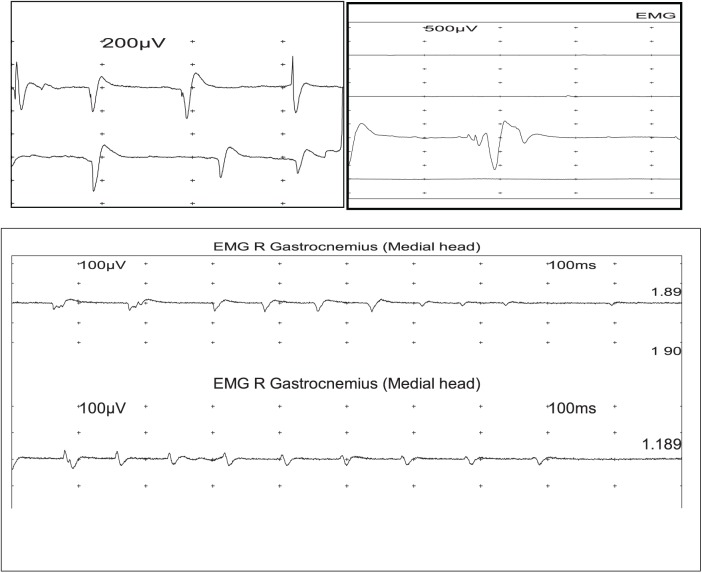
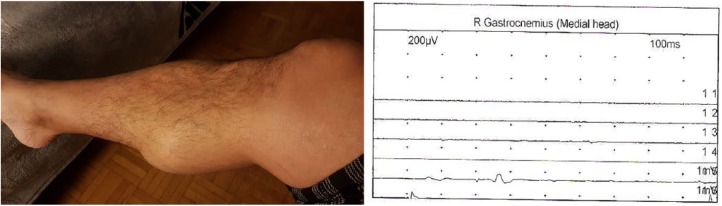
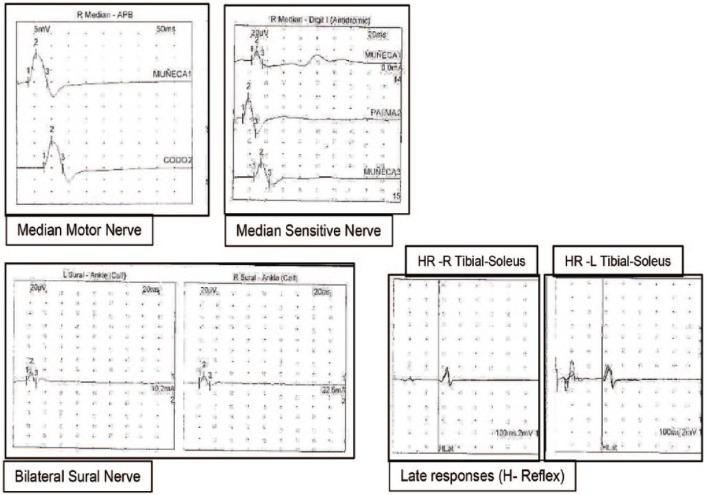
We report the case of a 46-years-old man with long-term asymptomatic hyperuricemia who started taking colchicine (0.5 mg/day) and allopurinol (100 mg/d) for normalization of biochemical values. After the third week of starting treatment, acute weakness was present; and by the fifth week, profound weakness in lower extremities and tenderness and cramps on thighs and calves with inability to climb stairs were also observed. Biochemical evaluation showed elevated muscle enzymes (creatinine kinase [CK] raised to five-folds its normal value) and electromyographic features were consistent with myopathy (at rest, fibrillations, positive sharp waves, high-frequency myotonic discharges; motor unit action potentials [MUAPs] of small amplitude, small duration, increased polyphasic Index and occasional satellite potentials; at maximal effort, interferential recruitment pattern with reduced amplitudes were observed). Normal motor and sensitive nerve conduction studies and normal late F-responses and H-reflex discarded neuropathy. Rapid improvement in muscle strength and prompt resolution of abnormal elevated muscle enzymes was observed after withdrawal of both medications. Colchicine is associated with some cases of myotoxicity but very small cases of colchicine-induced rhabdomyolysis are reported on the literature. Colchicine-induced rhabdomyolysis is related to the concomitant use of drugs (statins, steroids, erythromycin, and cyclosporine), renal, and/or hepatic impairment. To the best of our knowledge, this is an uncommon presentation of a case of colchicine-induced rhabdomyolysis reported in a patient without renal or hepatic dysfunction. Therefore, patients receiving colchicine even in the absence of renal insufficiency should be monitored for the development of myopathy and more rarely to rhabdomyolysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


