{"title":"来卡尼地平或来卡尼地平/依那普利联合用药对treatment-naïve期1或2期收缩期高血压患者血压的影响","authors":"Brian Rayner","doi":"10.2147/POR.S186070","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To describe the efficacy of a stratified approach on automatic office blood pressure (BP), 24-hour ambulatory BP, and BP variability (BPV) in treatment-naïve patients with systolic hypertension using lercanidipine for stage 1 and lercanidipine/enalapril for stage 2.</p><p><strong>Patients and methods: </strong>This was an open-label, prospective interventional study conducted in 22 general practices in South Africa. Treatment-naïve patients with stage 1 hypertension received lercanidipine 10 mg and patients with stage 2 received lercanidipine 10 mg/enalapril 10 mg. After 6 weeks, patients not reaching target (<140/90 mmHg) were up-titrated to lercanidipine 10 mg/enalapril 10 mg or lercanidipine 10 mg/enalapril 20 mg, respectively, for a further 6 weeks. Office BP was determined at each visit, and 24-hour ambulatory BP monitor (ABPM) at baseline and 12 weeks. The primary end point was changes in office BP, and secondary end points were changes in 24-hour ABPM and BPV.</p><p><strong>Results: </strong>Of the 198 patients, 48% had stage 1 and 52% stage 2 hypertension. The mean age was 55 years, body mass index was 29.2 kg/m<sup>2</sup>, 48.5% were female, and 15.1% were diabetic. The mean (SD) office SBP and DBP at baseline, 6 weeks, and 12 weeks was 158.2 (13.8), 141.6 (11.1), and 138.7 (16.7) mmHg (<i>P</i><0.00001), and 92.2 (10.6), 84.6 (11.1), and 82 (13.3) mmHg (<i>P</i><0.00001), respectively. The mean (SD) systolic and diastolic daytime ABPM at baseline and 12 weeks was 157 (16.63) and 142 (14.41) mmHg (<i>P</i><0.0001) and 88 (12.34) and 81 (10.79) mmHg (<i>P</i><0.0001), and the nighttime ABPM was 146 (15.68) and 133 (13.94) mmHg (<i>P</i><0.0001) and 79.5 (11.64) and 72.5 (10.05) mmHg (<i>P</i><0.009), respectively. There were few adverse events.</p><p><strong>Conclusion: </strong>Lercanidipine and lercanidipine/enalapril for stage 1 or 2 hypertension highly improves office SBP and DBP, overall 24-hour BP, daytime BP, and nighttime BP, also reducing BPV with few adverse effects.</p>","PeriodicalId":20399,"journal":{"name":"Pragmatic and Observational Research","volume":"10 ","pages":"9-14"},"PeriodicalIF":2.7000,"publicationDate":"2019-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/POR.S186070","citationCount":"0","resultStr":"{\"title\":\"The effect of lercanidipine or lercanidipine/enalapril combination on blood pressure in treatment-naïve patients with stage 1 or 2 systolic hypertension.\",\"authors\":\"Brian Rayner\",\"doi\":\"10.2147/POR.S186070\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To describe the efficacy of a stratified approach on automatic office blood pressure (BP), 24-hour ambulatory BP, and BP variability (BPV) in treatment-naïve patients with systolic hypertension using lercanidipine for stage 1 and lercanidipine/enalapril for stage 2.</p><p><strong>Patients and methods: </strong>This was an open-label, prospective interventional study conducted in 22 general practices in South Africa. Treatment-naïve patients with stage 1 hypertension received lercanidipine 10 mg and patients with stage 2 received lercanidipine 10 mg/enalapril 10 mg. After 6 weeks, patients not reaching target (<140/90 mmHg) were up-titrated to lercanidipine 10 mg/enalapril 10 mg or lercanidipine 10 mg/enalapril 20 mg, respectively, for a further 6 weeks. Office BP was determined at each visit, and 24-hour ambulatory BP monitor (ABPM) at baseline and 12 weeks. The primary end point was changes in office BP, and secondary end points were changes in 24-hour ABPM and BPV.</p><p><strong>Results: </strong>Of the 198 patients, 48% had stage 1 and 52% stage 2 hypertension. The mean age was 55 years, body mass index was 29.2 kg/m<sup>2</sup>, 48.5% were female, and 15.1% were diabetic. The mean (SD) office SBP and DBP at baseline, 6 weeks, and 12 weeks was 158.2 (13.8), 141.6 (11.1), and 138.7 (16.7) mmHg (<i>P</i><0.00001), and 92.2 (10.6), 84.6 (11.1), and 82 (13.3) mmHg (<i>P</i><0.00001), respectively. The mean (SD) systolic and diastolic daytime ABPM at baseline and 12 weeks was 157 (16.63) and 142 (14.41) mmHg (<i>P</i><0.0001) and 88 (12.34) and 81 (10.79) mmHg (<i>P</i><0.0001), and the nighttime ABPM was 146 (15.68) and 133 (13.94) mmHg (<i>P</i><0.0001) and 79.5 (11.64) and 72.5 (10.05) mmHg (<i>P</i><0.009), respectively. There were few adverse events.</p><p><strong>Conclusion: </strong>Lercanidipine and lercanidipine/enalapril for stage 1 or 2 hypertension highly improves office SBP and DBP, overall 24-hour BP, daytime BP, and nighttime BP, also reducing BPV with few adverse effects.</p>\",\"PeriodicalId\":20399,\"journal\":{\"name\":\"Pragmatic and Observational Research\",\"volume\":\"10 \",\"pages\":\"9-14\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2019-01-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.2147/POR.S186070\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pragmatic and Observational Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/POR.S186070\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pragmatic and Observational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/POR.S186070","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
The effect of lercanidipine or lercanidipine/enalapril combination on blood pressure in treatment-naïve patients with stage 1 or 2 systolic hypertension.
Purpose: To describe the efficacy of a stratified approach on automatic office blood pressure (BP), 24-hour ambulatory BP, and BP variability (BPV) in treatment-naïve patients with systolic hypertension using lercanidipine for stage 1 and lercanidipine/enalapril for stage 2.
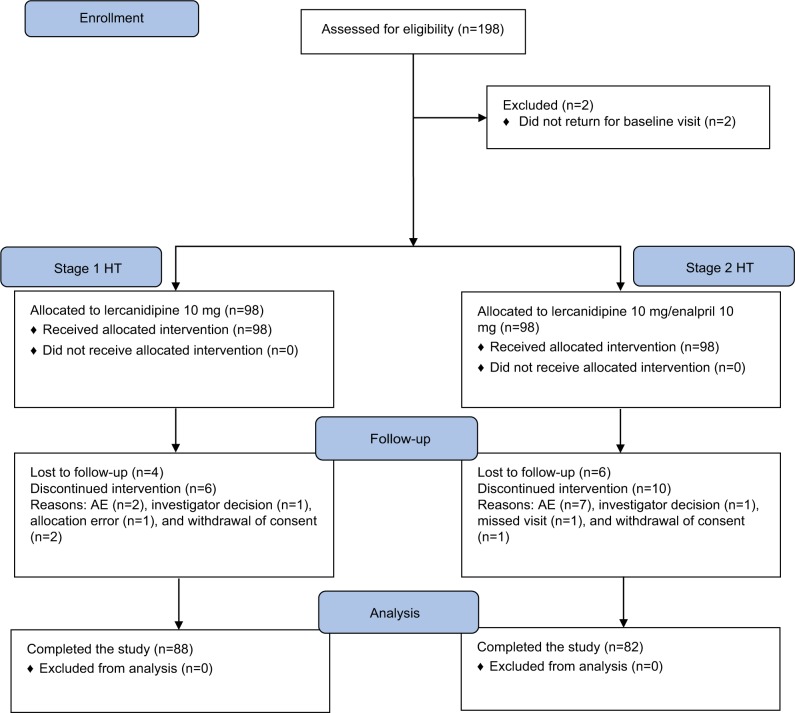
Patients and methods: This was an open-label, prospective interventional study conducted in 22 general practices in South Africa. Treatment-naïve patients with stage 1 hypertension received lercanidipine 10 mg and patients with stage 2 received lercanidipine 10 mg/enalapril 10 mg. After 6 weeks, patients not reaching target (<140/90 mmHg) were up-titrated to lercanidipine 10 mg/enalapril 10 mg or lercanidipine 10 mg/enalapril 20 mg, respectively, for a further 6 weeks. Office BP was determined at each visit, and 24-hour ambulatory BP monitor (ABPM) at baseline and 12 weeks. The primary end point was changes in office BP, and secondary end points were changes in 24-hour ABPM and BPV.
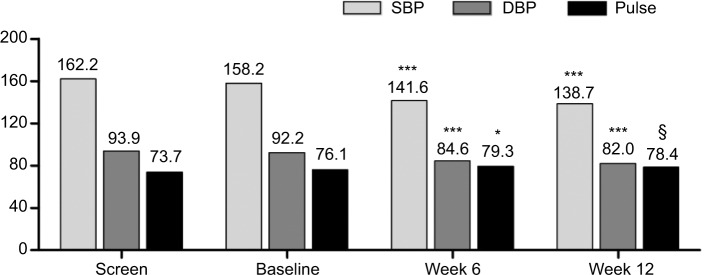
Results: Of the 198 patients, 48% had stage 1 and 52% stage 2 hypertension. The mean age was 55 years, body mass index was 29.2 kg/m2, 48.5% were female, and 15.1% were diabetic. The mean (SD) office SBP and DBP at baseline, 6 weeks, and 12 weeks was 158.2 (13.8), 141.6 (11.1), and 138.7 (16.7) mmHg (P<0.00001), and 92.2 (10.6), 84.6 (11.1), and 82 (13.3) mmHg (P<0.00001), respectively. The mean (SD) systolic and diastolic daytime ABPM at baseline and 12 weeks was 157 (16.63) and 142 (14.41) mmHg (P<0.0001) and 88 (12.34) and 81 (10.79) mmHg (P<0.0001), and the nighttime ABPM was 146 (15.68) and 133 (13.94) mmHg (P<0.0001) and 79.5 (11.64) and 72.5 (10.05) mmHg (P<0.009), respectively. There were few adverse events.
Conclusion: Lercanidipine and lercanidipine/enalapril for stage 1 or 2 hypertension highly improves office SBP and DBP, overall 24-hour BP, daytime BP, and nighttime BP, also reducing BPV with few adverse effects.
期刊介绍:
Pragmatic and Observational Research is an international, peer-reviewed, open-access journal that publishes data from studies designed to closely reflect medical interventions in real-world clinical practice, providing insights beyond classical randomized controlled trials (RCTs). While RCTs maximize internal validity for cause-and-effect relationships, they often represent only specific patient groups. This journal aims to complement such studies by providing data that better mirrors real-world patients and the usage of medicines, thus informing guidelines and enhancing the applicability of research findings across diverse patient populations encountered in everyday clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


