Wilfredo De Jesus-Rojas, Ricardo A Mosquera, Cheryl Samuels, Julie Eapen, Traci Gonzales, Tomika Harris, Sandra McKay, Fatima Boricha, Claudia Pedroza, Chiamaka Aneji, Amir Khan, Cindy Jon, Katrina McBeth, James Stark, Aravind Yadav, Jon E Tyson
{"title":"综合医疗护理对新生儿重症监护病房气管切开术患儿远期预后的影响。","authors":"Wilfredo De Jesus-Rojas, Ricardo A Mosquera, Cheryl Samuels, Julie Eapen, Traci Gonzales, Tomika Harris, Sandra McKay, Fatima Boricha, Claudia Pedroza, Chiamaka Aneji, Amir Khan, Cindy Jon, Katrina McBeth, James Stark, Aravind Yadav, Jon E Tyson","doi":"10.2174/1874306401812010039","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Survival of infants with complex care has led to a growing population of technology-dependent children. Medical technology introduces additional complexity to patient care. Outcomes after NICU discharge comparing Usual Care (UC) with Comprehensive Care (CC) remain elusive.</p><p><strong>Objective: </strong>To compare the outcomes of technology-dependent infants discharged from NICU with tracheostomy following UC versus CC.</p><p><strong>Methods: </strong>A single site retrospective study evaluated forty-three (N=43) technology-dependent infants discharged from NICU with tracheostomy over 5½ years (2011-2017). CC provided 24-hour accessible healthcare-providers using an enhanced medical home. Mortality, total hospital admissions, 30-days readmission rate, time-to-mechanical ventilation liberation, and time-to-decannulation were compared between groups.</p><p><strong>Results: </strong>CC group showed significantly lower mortality (3.4%) versus UC (35.7%), RR, 0.09 [95%CI, 0.12-0.75], P=0.025. CC reduced total hospital admissions to 78 per 100 child-years versus 162 for UC; RR, 0.48 [95% CI, 0.25-0.93], P=0.03. The 30-day readmission rate was 21% compared to 36% in UC; RR, 0.58 [95% CI, 0.21-1.58], P=0.29). In competing-risk regression analysis (treating death as a competing-risk), hazard of having mechanical ventilation removal in CC was two times higher than UC; SHR, 2.19 [95% CI, 0.70-6.84]. There was no difference in time-to-decannulation between groups; SHR, 1.09 [95% CI, 0.37-3.15].</p><p><strong>Conclusion: </strong>CC significantly decreased mortality, total number of hospital admissions and length of time-to-mechanical ventilation liberation.</p>","PeriodicalId":39127,"journal":{"name":"Open Respiratory Medicine Journal","volume":"12 ","pages":"39-49"},"PeriodicalIF":0.0000,"publicationDate":"2018-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6110063/pdf/","citationCount":"11","resultStr":"{\"title\":\"The Effect of Comprehensive Medical Care on the Long-Term Outcomes of Children Discharged from the NICU with Tracheostomy.\",\"authors\":\"Wilfredo De Jesus-Rojas, Ricardo A Mosquera, Cheryl Samuels, Julie Eapen, Traci Gonzales, Tomika Harris, Sandra McKay, Fatima Boricha, Claudia Pedroza, Chiamaka Aneji, Amir Khan, Cindy Jon, Katrina McBeth, James Stark, Aravind Yadav, Jon E Tyson\",\"doi\":\"10.2174/1874306401812010039\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Survival of infants with complex care has led to a growing population of technology-dependent children. Medical technology introduces additional complexity to patient care. Outcomes after NICU discharge comparing Usual Care (UC) with Comprehensive Care (CC) remain elusive.</p><p><strong>Objective: </strong>To compare the outcomes of technology-dependent infants discharged from NICU with tracheostomy following UC versus CC.</p><p><strong>Methods: </strong>A single site retrospective study evaluated forty-three (N=43) technology-dependent infants discharged from NICU with tracheostomy over 5½ years (2011-2017). CC provided 24-hour accessible healthcare-providers using an enhanced medical home. Mortality, total hospital admissions, 30-days readmission rate, time-to-mechanical ventilation liberation, and time-to-decannulation were compared between groups.</p><p><strong>Results: </strong>CC group showed significantly lower mortality (3.4%) versus UC (35.7%), RR, 0.09 [95%CI, 0.12-0.75], P=0.025. CC reduced total hospital admissions to 78 per 100 child-years versus 162 for UC; RR, 0.48 [95% CI, 0.25-0.93], P=0.03. The 30-day readmission rate was 21% compared to 36% in UC; RR, 0.58 [95% CI, 0.21-1.58], P=0.29). In competing-risk regression analysis (treating death as a competing-risk), hazard of having mechanical ventilation removal in CC was two times higher than UC; SHR, 2.19 [95% CI, 0.70-6.84]. There was no difference in time-to-decannulation between groups; SHR, 1.09 [95% CI, 0.37-3.15].</p><p><strong>Conclusion: </strong>CC significantly decreased mortality, total number of hospital admissions and length of time-to-mechanical ventilation liberation.</p>\",\"PeriodicalId\":39127,\"journal\":{\"name\":\"Open Respiratory Medicine Journal\",\"volume\":\"12 \",\"pages\":\"39-49\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-07-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6110063/pdf/\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Respiratory Medicine Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2174/1874306401812010039\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Respiratory Medicine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2174/1874306401812010039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
The Effect of Comprehensive Medical Care on the Long-Term Outcomes of Children Discharged from the NICU with Tracheostomy.
Background: Survival of infants with complex care has led to a growing population of technology-dependent children. Medical technology introduces additional complexity to patient care. Outcomes after NICU discharge comparing Usual Care (UC) with Comprehensive Care (CC) remain elusive.
Objective: To compare the outcomes of technology-dependent infants discharged from NICU with tracheostomy following UC versus CC.
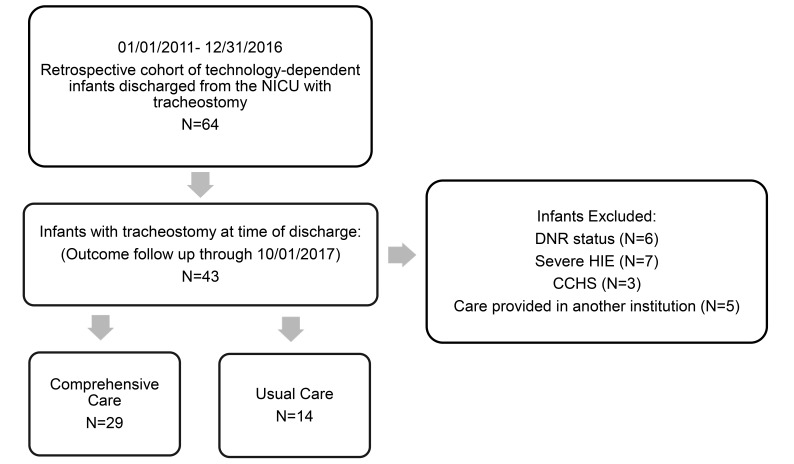
Methods: A single site retrospective study evaluated forty-three (N=43) technology-dependent infants discharged from NICU with tracheostomy over 5½ years (2011-2017). CC provided 24-hour accessible healthcare-providers using an enhanced medical home. Mortality, total hospital admissions, 30-days readmission rate, time-to-mechanical ventilation liberation, and time-to-decannulation were compared between groups.
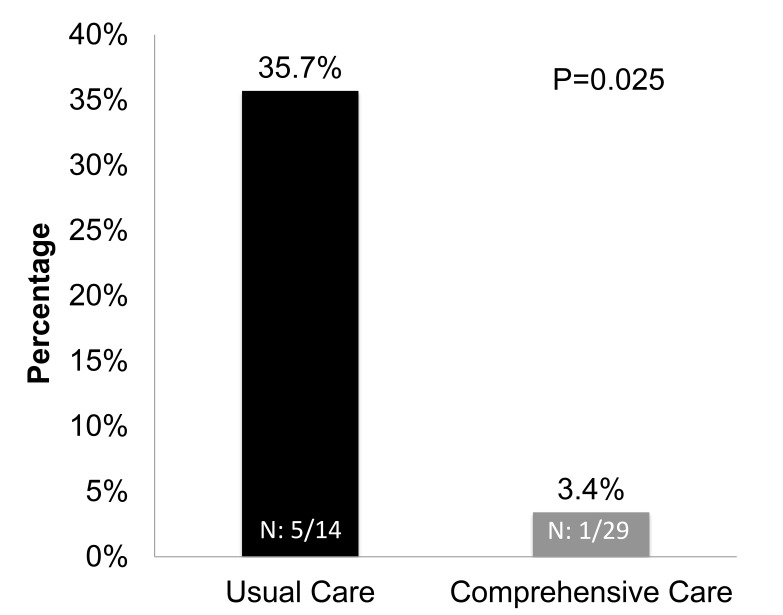
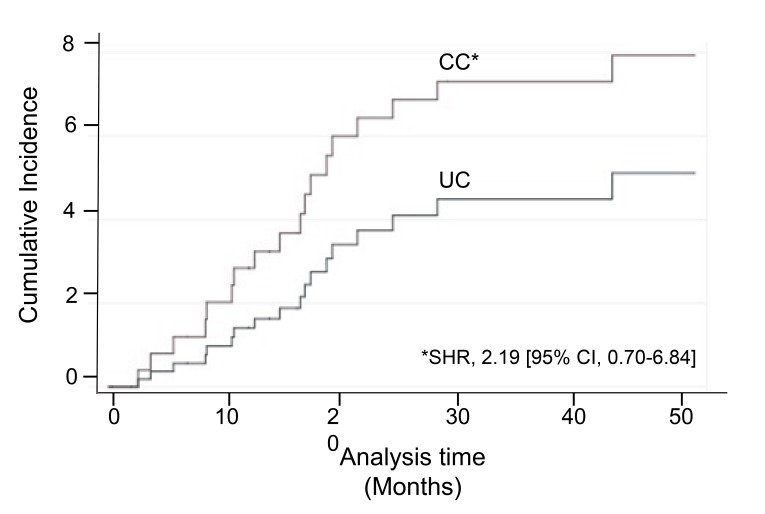
Results: CC group showed significantly lower mortality (3.4%) versus UC (35.7%), RR, 0.09 [95%CI, 0.12-0.75], P=0.025. CC reduced total hospital admissions to 78 per 100 child-years versus 162 for UC; RR, 0.48 [95% CI, 0.25-0.93], P=0.03. The 30-day readmission rate was 21% compared to 36% in UC; RR, 0.58 [95% CI, 0.21-1.58], P=0.29). In competing-risk regression analysis (treating death as a competing-risk), hazard of having mechanical ventilation removal in CC was two times higher than UC; SHR, 2.19 [95% CI, 0.70-6.84]. There was no difference in time-to-decannulation between groups; SHR, 1.09 [95% CI, 0.37-3.15].
Conclusion: CC significantly decreased mortality, total number of hospital admissions and length of time-to-mechanical ventilation liberation.
期刊介绍:
The Open Respiratory Medicine Journal is an Open Access online journal, which publishes research articles, reviews/mini-reviews, letters and guest edited single topic issues in all important areas of experimental and clinical research in respiratory medicine. Topics covered include: -COPD- Occupational disorders, and the role of allergens and pollutants- Asthma- Allergy- Non-invasive ventilation- Therapeutic intervention- Lung cancer- Lung infections respiratory diseases- Therapeutic interventions- Adult and paediatric medicine- Cell biology. The Open Respiratory Medicine Journal, a peer reviewed journal, is an important and reliable source of current information on important recent developments in the field. The emphasis will be on publishing quality articles rapidly and making them freely available worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


