{"title":"内镜下成功治疗食管切除术后难治性反流:第一例临床病例。","authors":"Hirotsugu Nagase, Makoto Yamasaki, Yoshitomo Yanagimoto, Takashi Kanemura, Shigeyoshi Higashi, Kota Momose, Ryo Kato, Yasuhiro Miyazaki, Tomoki Makino, Tsuyoshi Takahashi, Yukinori Kurokawa, Hiroshi Miyata, Shuji Takiguchi, Masaki Mori, Yuichiro Doki, Kiyokazu Nakajima","doi":"10.1177/1179552218784946","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The reflux of duodeno-gastric contents into the remnant esophagus (gastric tube-esophageal reflux: GTER) is a significant issues in long-term esophageal cancer survivors after radical esophagectomy. We attempted endoscopic valve (funnel) creation for prevention for GTER using OverStitch endoscopic suturing system.</p><p><strong>Methods: </strong>The OverStitch was mounted onto a standard double-channel endoscope. Under general anesthesia, the funnel creation was attempted by placing semi-full thickness sutures on the gastric wall, at 3 cm distal to the primary esophago-gastric anastomosis. The postoperative outcomes were also evaluated.</p><p><strong>Results: </strong>In total, 4 sutures were needed and the operating time was 62 minutes without complication. The endoscopic and swallowing studies, as well as pH profile, were all improved postoperatively. The patient's quality of life was dramatically improved with complete disappearance of night-time reflux in spine position.</p><p><strong>Conclusions: </strong>Endoscopic antireflux funnel creation was feasible and safe. This procedure may become a useful treatment for patients with severe GTER after esophagectomy.</p>","PeriodicalId":10382,"journal":{"name":"Clinical Medicine Insights. Gastroenterology","volume":" ","pages":"1179552218784946"},"PeriodicalIF":0.0000,"publicationDate":"2018-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179552218784946","citationCount":"3","resultStr":"{\"title\":\"Successful Endoscopic Treatment of Post-esophagectomy Refractory Reflux Using OverStitch: The First Clinical Case.\",\"authors\":\"Hirotsugu Nagase, Makoto Yamasaki, Yoshitomo Yanagimoto, Takashi Kanemura, Shigeyoshi Higashi, Kota Momose, Ryo Kato, Yasuhiro Miyazaki, Tomoki Makino, Tsuyoshi Takahashi, Yukinori Kurokawa, Hiroshi Miyata, Shuji Takiguchi, Masaki Mori, Yuichiro Doki, Kiyokazu Nakajima\",\"doi\":\"10.1177/1179552218784946\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The reflux of duodeno-gastric contents into the remnant esophagus (gastric tube-esophageal reflux: GTER) is a significant issues in long-term esophageal cancer survivors after radical esophagectomy. We attempted endoscopic valve (funnel) creation for prevention for GTER using OverStitch endoscopic suturing system.</p><p><strong>Methods: </strong>The OverStitch was mounted onto a standard double-channel endoscope. Under general anesthesia, the funnel creation was attempted by placing semi-full thickness sutures on the gastric wall, at 3 cm distal to the primary esophago-gastric anastomosis. The postoperative outcomes were also evaluated.</p><p><strong>Results: </strong>In total, 4 sutures were needed and the operating time was 62 minutes without complication. The endoscopic and swallowing studies, as well as pH profile, were all improved postoperatively. The patient's quality of life was dramatically improved with complete disappearance of night-time reflux in spine position.</p><p><strong>Conclusions: </strong>Endoscopic antireflux funnel creation was feasible and safe. This procedure may become a useful treatment for patients with severe GTER after esophagectomy.</p>\",\"PeriodicalId\":10382,\"journal\":{\"name\":\"Clinical Medicine Insights. Gastroenterology\",\"volume\":\" \",\"pages\":\"1179552218784946\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-07-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179552218784946\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179552218784946\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179552218784946","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Successful Endoscopic Treatment of Post-esophagectomy Refractory Reflux Using OverStitch: The First Clinical Case.
Aims: The reflux of duodeno-gastric contents into the remnant esophagus (gastric tube-esophageal reflux: GTER) is a significant issues in long-term esophageal cancer survivors after radical esophagectomy. We attempted endoscopic valve (funnel) creation for prevention for GTER using OverStitch endoscopic suturing system.
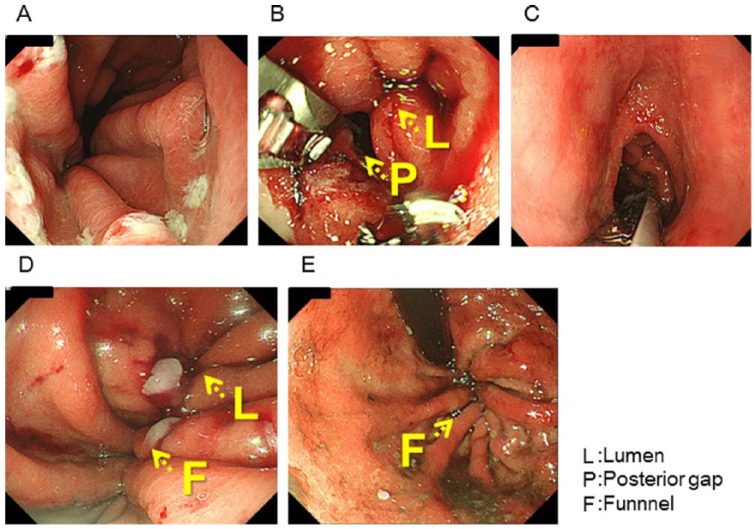
Methods: The OverStitch was mounted onto a standard double-channel endoscope. Under general anesthesia, the funnel creation was attempted by placing semi-full thickness sutures on the gastric wall, at 3 cm distal to the primary esophago-gastric anastomosis. The postoperative outcomes were also evaluated.
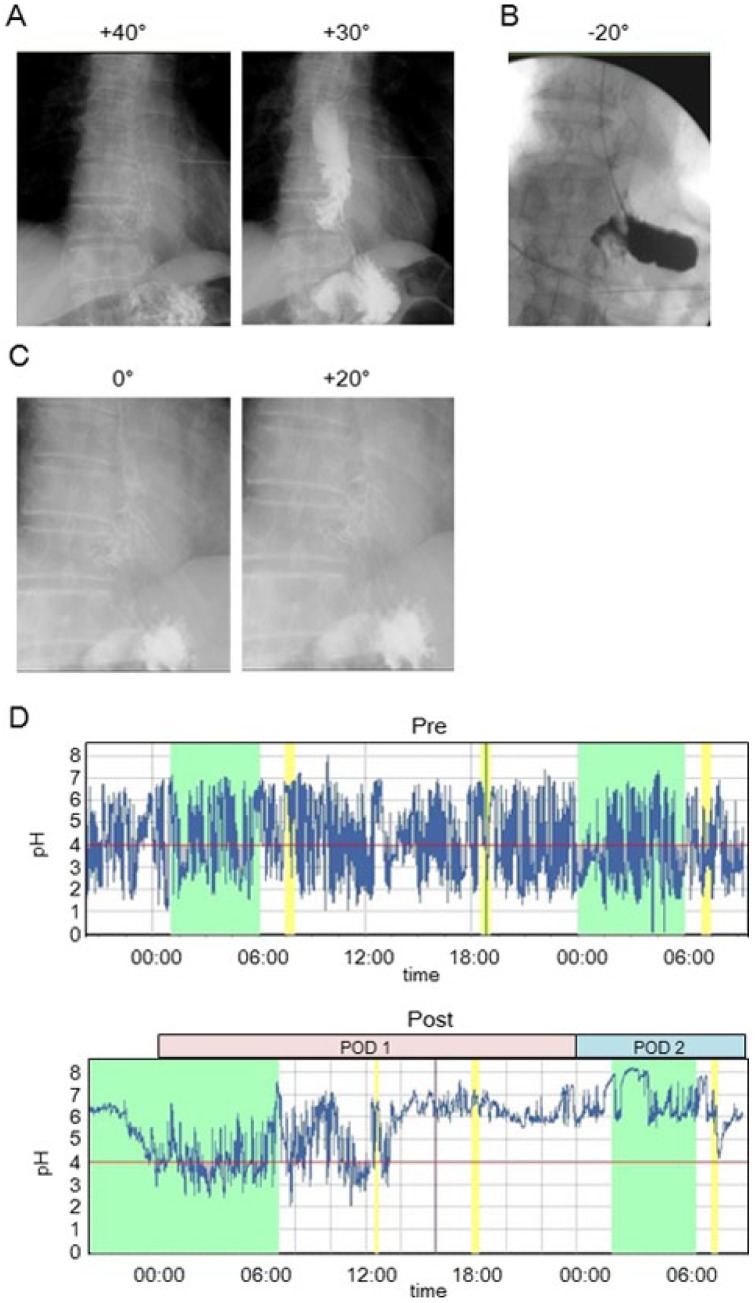
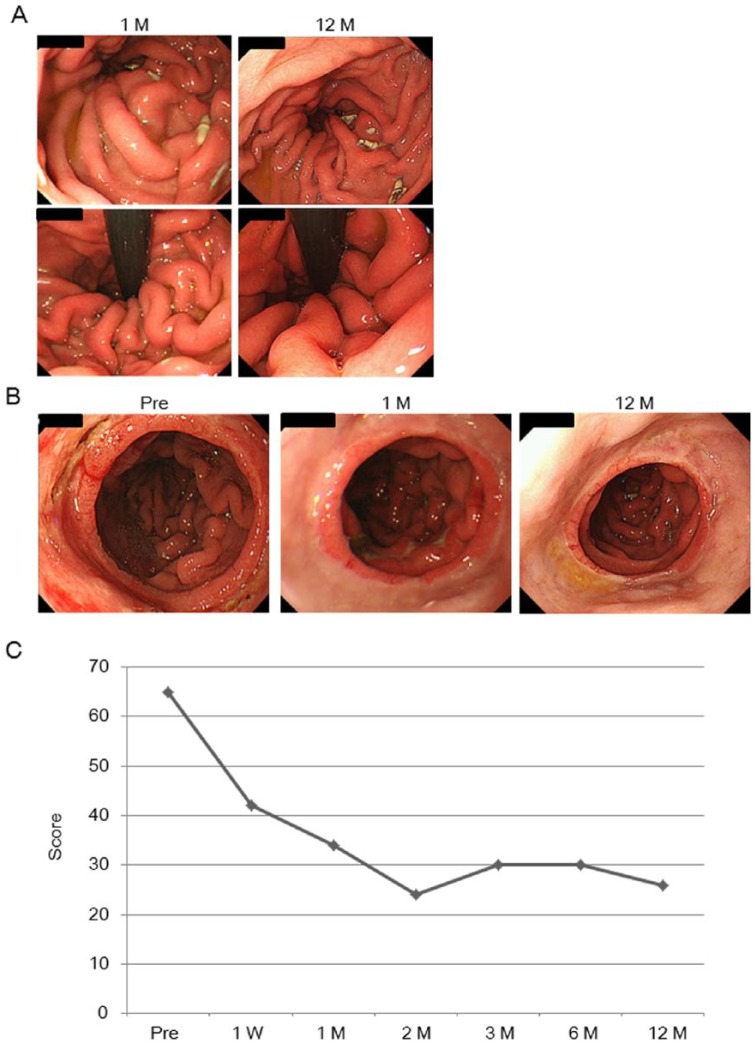
Results: In total, 4 sutures were needed and the operating time was 62 minutes without complication. The endoscopic and swallowing studies, as well as pH profile, were all improved postoperatively. The patient's quality of life was dramatically improved with complete disappearance of night-time reflux in spine position.
Conclusions: Endoscopic antireflux funnel creation was feasible and safe. This procedure may become a useful treatment for patients with severe GTER after esophagectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


