Hussein A Algahtani, Basim W Sait, Bader H Shirah, Majed A Almuraee
{"title":"双重病理引起的产后头痛:给麻醉师的信息。","authors":"Hussein A Algahtani, Basim W Sait, Bader H Shirah, Majed A Almuraee","doi":"10.17712/nsj.2018.3.20180489","DOIUrl":null,"url":null,"abstract":"P is the collection of air within the cranial cavity. It was first described by Thomas Du in 1866 in an autopsy report of a trauma patient. In 1914, Wolff was the first to use the term pneumocephalus. Published studies and reviews indicated that trauma and surgery are the most common causes of pneumocephalus accounting for 75-90% of cases. In addition, neoplasms account for 13% and infections account for 9% of cases. Other causes include lumbar puncture, angiography, Valsalva’s maneuver, subarachnoid-pleural fistula, congenital skull defects, basilar skull fractures, sinus fractures, osteoma, central venous catheterization, epidural steroid injections, and epidural anesthesia. Spontaneous or idiopathic pneumocephalus was only found in 0.6% of the cases.1,2 In this article, we aim to report a case of post-dural puncture headache and pneumocephalus complicating epidural analgesia using the loss of resistance to air technique. Post-epidural puncture headache was successfully treated with an autologous blood patch. However, headache persisted, and another cause was investigated further. This patient was found to have both post-dural puncture headache and pneumocephalus. A 36-year-old female delivered a healthy male infant 24 hours prior to presentation through a spontaneous vaginal delivery. She received an epidural analgesia using Tuohy needle 18 gauge for labor pain. Immediately after the epidural injection, she developed a severe headache which was constant and throbbing in nature located in both frontal and occipital regions with radiation to the neck. Due to labor pain and being occupied by giving birth, she did not complain about this headache except after delivery. The pain was worse with sitting or standing up and relieved by lying flat. The pain was not similar to her usual migraine headaches, which started at the age of 16. There were no associated fever, photophobia, neck stiffens, sensory symptoms, or weakness. There was no nasal discharge, epistaxis, anosmia, facial pain, or ear discharge. Her past surgical history was remarkable for previous varicose vein surgery, which was carried out 3 years ago under local anesthesia. During this admission, there was no history of cannulation of major arteries or veins in the neck. She had 2 previous pregnancies that were uneventful. On examination, her vital signs were normal. She was in severe pain, and she liked to stay in a supine position. Her neurological examination showed a normal higher mental functions, cranial nerve examination, motor, sensory and coordination systems. Her gait was not assessed, and her fundus was normal. There were no signs of meningeal irritation. Her basic blood work including chemistry was normal. The patient was treated conservatively using intravenous hydration, non-steroidal anti-inflammatory drugs, and caffeine. Twenty-four hours later, she continued to be symptomatic, and an epidural autologous blood patch (22 cc) was carried out by the same anesthesia consultant who performed the initial epidural anesthesia with some improvement in her symptoms. The patient started to walk with disappearance of the postural headache despite having a constant headache in the frontal region of her head that had no precipitating or aggravating factors. Cerebrospinal fluid (CSF) analysis was normal including opening pressure, physical appearance, and analysis. Computed tomography (CT) of the brain with CT venography was carried out to rule out secondary headache disorders showed pockets of air within the lateral ventricles, diagnostic of pneumocephalus (Figure 1). The patient gradually improved and discharged home 24 hours later. On a visit to the clinic 2 weeks later, she was free of pain with a normal clinical examination. The pathophysiology of pneumocephalus involves several mechanisms based on the cause or underlying condition. Several mechanisms may work simultaneously in the same patient. Pneumocephalus may be due to an excessive leak of the CSF causing intracranial hypotension. As a result, air is drawn into the cranial cavity similar to the entry of air into an inverted bottle of water as the fluid escapes. This mechanism is considered the most common during neurosurgical and anesthesia procedures. The second mechanism may involve ball-valve effect with air being forced through the area of intracranial dural defect from sudden changes in nasopharyngeal pressure such as during coughing or sneezing. Other mechanisms of pneumocephalus include the admission of air into the cranium from penetrating skull injuries and intracranial infection from gas-forming organisms resulting in intracerebral gas collection.4 Pneumocephalus is usually a benign and self-limiting condition with the air being spontaneously absorbed without producing symptoms. However, if the air accumulates in the brain or the cranium, elevated intracranial pressure and neurological","PeriodicalId":520723,"journal":{"name":"Neurosciences (Riyadh, Saudi Arabia)","volume":" ","pages":"262-264"},"PeriodicalIF":1.3000,"publicationDate":"2018-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/6a/Neurosciences-23-262.PMC8015576.pdf","citationCount":"1","resultStr":"{\"title\":\"Post-partum headache caused by dual pathology: A message to the anesthetist.\",\"authors\":\"Hussein A Algahtani, Basim W Sait, Bader H Shirah, Majed A Almuraee\",\"doi\":\"10.17712/nsj.2018.3.20180489\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"P is the collection of air within the cranial cavity. It was first described by Thomas Du in 1866 in an autopsy report of a trauma patient. In 1914, Wolff was the first to use the term pneumocephalus. Published studies and reviews indicated that trauma and surgery are the most common causes of pneumocephalus accounting for 75-90% of cases. In addition, neoplasms account for 13% and infections account for 9% of cases. Other causes include lumbar puncture, angiography, Valsalva’s maneuver, subarachnoid-pleural fistula, congenital skull defects, basilar skull fractures, sinus fractures, osteoma, central venous catheterization, epidural steroid injections, and epidural anesthesia. Spontaneous or idiopathic pneumocephalus was only found in 0.6% of the cases.1,2 In this article, we aim to report a case of post-dural puncture headache and pneumocephalus complicating epidural analgesia using the loss of resistance to air technique. Post-epidural puncture headache was successfully treated with an autologous blood patch. However, headache persisted, and another cause was investigated further. This patient was found to have both post-dural puncture headache and pneumocephalus. A 36-year-old female delivered a healthy male infant 24 hours prior to presentation through a spontaneous vaginal delivery. She received an epidural analgesia using Tuohy needle 18 gauge for labor pain. Immediately after the epidural injection, she developed a severe headache which was constant and throbbing in nature located in both frontal and occipital regions with radiation to the neck. Due to labor pain and being occupied by giving birth, she did not complain about this headache except after delivery. The pain was worse with sitting or standing up and relieved by lying flat. The pain was not similar to her usual migraine headaches, which started at the age of 16. There were no associated fever, photophobia, neck stiffens, sensory symptoms, or weakness. There was no nasal discharge, epistaxis, anosmia, facial pain, or ear discharge. Her past surgical history was remarkable for previous varicose vein surgery, which was carried out 3 years ago under local anesthesia. During this admission, there was no history of cannulation of major arteries or veins in the neck. She had 2 previous pregnancies that were uneventful. On examination, her vital signs were normal. She was in severe pain, and she liked to stay in a supine position. Her neurological examination showed a normal higher mental functions, cranial nerve examination, motor, sensory and coordination systems. Her gait was not assessed, and her fundus was normal. There were no signs of meningeal irritation. Her basic blood work including chemistry was normal. The patient was treated conservatively using intravenous hydration, non-steroidal anti-inflammatory drugs, and caffeine. Twenty-four hours later, she continued to be symptomatic, and an epidural autologous blood patch (22 cc) was carried out by the same anesthesia consultant who performed the initial epidural anesthesia with some improvement in her symptoms. The patient started to walk with disappearance of the postural headache despite having a constant headache in the frontal region of her head that had no precipitating or aggravating factors. Cerebrospinal fluid (CSF) analysis was normal including opening pressure, physical appearance, and analysis. Computed tomography (CT) of the brain with CT venography was carried out to rule out secondary headache disorders showed pockets of air within the lateral ventricles, diagnostic of pneumocephalus (Figure 1). The patient gradually improved and discharged home 24 hours later. On a visit to the clinic 2 weeks later, she was free of pain with a normal clinical examination. The pathophysiology of pneumocephalus involves several mechanisms based on the cause or underlying condition. Several mechanisms may work simultaneously in the same patient. Pneumocephalus may be due to an excessive leak of the CSF causing intracranial hypotension. As a result, air is drawn into the cranial cavity similar to the entry of air into an inverted bottle of water as the fluid escapes. This mechanism is considered the most common during neurosurgical and anesthesia procedures. The second mechanism may involve ball-valve effect with air being forced through the area of intracranial dural defect from sudden changes in nasopharyngeal pressure such as during coughing or sneezing. Other mechanisms of pneumocephalus include the admission of air into the cranium from penetrating skull injuries and intracranial infection from gas-forming organisms resulting in intracerebral gas collection.4 Pneumocephalus is usually a benign and self-limiting condition with the air being spontaneously absorbed without producing symptoms. However, if the air accumulates in the brain or the cranium, elevated intracranial pressure and neurological\",\"PeriodicalId\":520723,\"journal\":{\"name\":\"Neurosciences (Riyadh, Saudi Arabia)\",\"volume\":\" \",\"pages\":\"262-264\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2018-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/6a/Neurosciences-23-262.PMC8015576.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurosciences (Riyadh, Saudi Arabia)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.17712/nsj.2018.3.20180489\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosciences (Riyadh, Saudi Arabia)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.17712/nsj.2018.3.20180489","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Post-partum headache caused by dual pathology: A message to the anesthetist.
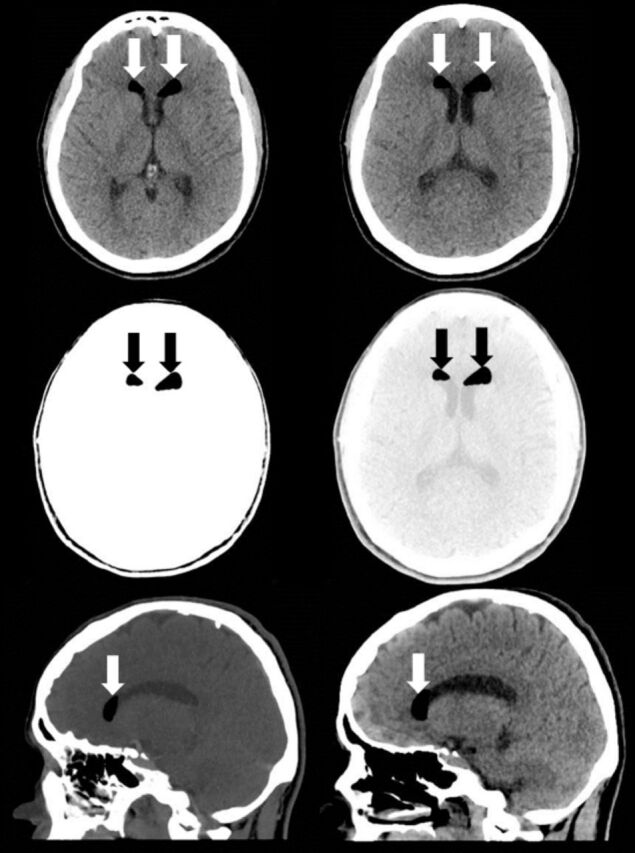
P is the collection of air within the cranial cavity. It was first described by Thomas Du in 1866 in an autopsy report of a trauma patient. In 1914, Wolff was the first to use the term pneumocephalus. Published studies and reviews indicated that trauma and surgery are the most common causes of pneumocephalus accounting for 75-90% of cases. In addition, neoplasms account for 13% and infections account for 9% of cases. Other causes include lumbar puncture, angiography, Valsalva’s maneuver, subarachnoid-pleural fistula, congenital skull defects, basilar skull fractures, sinus fractures, osteoma, central venous catheterization, epidural steroid injections, and epidural anesthesia. Spontaneous or idiopathic pneumocephalus was only found in 0.6% of the cases.1,2 In this article, we aim to report a case of post-dural puncture headache and pneumocephalus complicating epidural analgesia using the loss of resistance to air technique. Post-epidural puncture headache was successfully treated with an autologous blood patch. However, headache persisted, and another cause was investigated further. This patient was found to have both post-dural puncture headache and pneumocephalus. A 36-year-old female delivered a healthy male infant 24 hours prior to presentation through a spontaneous vaginal delivery. She received an epidural analgesia using Tuohy needle 18 gauge for labor pain. Immediately after the epidural injection, she developed a severe headache which was constant and throbbing in nature located in both frontal and occipital regions with radiation to the neck. Due to labor pain and being occupied by giving birth, she did not complain about this headache except after delivery. The pain was worse with sitting or standing up and relieved by lying flat. The pain was not similar to her usual migraine headaches, which started at the age of 16. There were no associated fever, photophobia, neck stiffens, sensory symptoms, or weakness. There was no nasal discharge, epistaxis, anosmia, facial pain, or ear discharge. Her past surgical history was remarkable for previous varicose vein surgery, which was carried out 3 years ago under local anesthesia. During this admission, there was no history of cannulation of major arteries or veins in the neck. She had 2 previous pregnancies that were uneventful. On examination, her vital signs were normal. She was in severe pain, and she liked to stay in a supine position. Her neurological examination showed a normal higher mental functions, cranial nerve examination, motor, sensory and coordination systems. Her gait was not assessed, and her fundus was normal. There were no signs of meningeal irritation. Her basic blood work including chemistry was normal. The patient was treated conservatively using intravenous hydration, non-steroidal anti-inflammatory drugs, and caffeine. Twenty-four hours later, she continued to be symptomatic, and an epidural autologous blood patch (22 cc) was carried out by the same anesthesia consultant who performed the initial epidural anesthesia with some improvement in her symptoms. The patient started to walk with disappearance of the postural headache despite having a constant headache in the frontal region of her head that had no precipitating or aggravating factors. Cerebrospinal fluid (CSF) analysis was normal including opening pressure, physical appearance, and analysis. Computed tomography (CT) of the brain with CT venography was carried out to rule out secondary headache disorders showed pockets of air within the lateral ventricles, diagnostic of pneumocephalus (Figure 1). The patient gradually improved and discharged home 24 hours later. On a visit to the clinic 2 weeks later, she was free of pain with a normal clinical examination. The pathophysiology of pneumocephalus involves several mechanisms based on the cause or underlying condition. Several mechanisms may work simultaneously in the same patient. Pneumocephalus may be due to an excessive leak of the CSF causing intracranial hypotension. As a result, air is drawn into the cranial cavity similar to the entry of air into an inverted bottle of water as the fluid escapes. This mechanism is considered the most common during neurosurgical and anesthesia procedures. The second mechanism may involve ball-valve effect with air being forced through the area of intracranial dural defect from sudden changes in nasopharyngeal pressure such as during coughing or sneezing. Other mechanisms of pneumocephalus include the admission of air into the cranium from penetrating skull injuries and intracranial infection from gas-forming organisms resulting in intracerebral gas collection.4 Pneumocephalus is usually a benign and self-limiting condition with the air being spontaneously absorbed without producing symptoms. However, if the air accumulates in the brain or the cranium, elevated intracranial pressure and neurological

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


