Robert A Moran, Sindhu Barola, Joanna K Law, Stuart K Amateau, Daniil Rolshud, Erin Corless, Vandhana Kiswani, Vikesh K Singh, Anthony N Kalloo, Mouen A Khashab, Anne Marie Lennon, Patrick I Okolo, Vivek Kumbhari
{"title":"一项随机对照试验比较了前行单球囊与螺旋肠镜的最大插入深度。","authors":"Robert A Moran, Sindhu Barola, Joanna K Law, Stuart K Amateau, Daniil Rolshud, Erin Corless, Vandhana Kiswani, Vikesh K Singh, Anthony N Kalloo, Mouen A Khashab, Anne Marie Lennon, Patrick I Okolo, Vivek Kumbhari","doi":"10.1177/1179552218754881","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Three device-assisted deep endoscopic platforms presently exist and are available for clinical use: double-balloon enteroscopy, single-balloon enteroscopy (SBE), and spiral enteroscopy (SE). In a retrospective study, SE was associated with a greater depth of maximal insertion (DMI) with similar diagnostic yields and procedure time as compared with SBE.</p><p><strong>Aims: </strong>This was a prospective, randomized comparison of SE and SBE with respect to DMI, diagnostic yield, procedure time, and rate of adverse events.</p><p><strong>Methods: </strong>Patients were prospectively randomized to undergo either anterograde SE or SBE. Patient demographics, indication for procedure, DMI, procedure time, therapeutic procedure time, adverse event, diagnostic findings, and therapeutic interventions were prospectively recorded. The primary outcome was DMI. Secondary outcomes included: procedure time; diagnostic yield; therapeutic yield and adverse event rates.</p><p><strong>Results: </strong>During the study period, 30 patients underwent deep enteroscopy (SE 13, SBE 17). The most common indication was gastrointestinal bleeding in both groups. There was no significant difference in the DMI between SE and SBE (330.0 ± 88.2 cm vs 285.3 ± 80.8 cm, <i>P</i> = .16). There was no difference between SE and SBE in procedure time (37.0 ± 10.5 vs 38.3 ± 12.4, <i>P</i> = .76), diagnostic yield (SE = 9 [69%] vs SBE = 7 [41%], <i>P</i> = .16), or therapeutic yield (SE = 6 [46%] vs SBE = 4 [24%], <i>P</i> = .26). There were no major adverse events in either group.</p><p><strong>Conclusions: </strong>Spiral enteroscopy and SBE are similar with respect to DMI, diagnostic yield, therapeutic yield, procedure time, and rate of adverse events. Small numbers prevent giving a definitive judgment and future adequately powered prospective study is required to confirm these findings.</p>","PeriodicalId":10382,"journal":{"name":"Clinical Medicine Insights. Gastroenterology","volume":" ","pages":"1179552218754881"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/aa/10.1177_1179552218754881.PMC5788085.pdf","citationCount":"0","resultStr":"{\"title\":\"A Randomized Controlled Trial Comparing the Depth of Maximal Insertion Between Anterograde Single-Balloon Versus Spiral Enteroscopy.\",\"authors\":\"Robert A Moran, Sindhu Barola, Joanna K Law, Stuart K Amateau, Daniil Rolshud, Erin Corless, Vandhana Kiswani, Vikesh K Singh, Anthony N Kalloo, Mouen A Khashab, Anne Marie Lennon, Patrick I Okolo, Vivek Kumbhari\",\"doi\":\"10.1177/1179552218754881\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Three device-assisted deep endoscopic platforms presently exist and are available for clinical use: double-balloon enteroscopy, single-balloon enteroscopy (SBE), and spiral enteroscopy (SE). In a retrospective study, SE was associated with a greater depth of maximal insertion (DMI) with similar diagnostic yields and procedure time as compared with SBE.</p><p><strong>Aims: </strong>This was a prospective, randomized comparison of SE and SBE with respect to DMI, diagnostic yield, procedure time, and rate of adverse events.</p><p><strong>Methods: </strong>Patients were prospectively randomized to undergo either anterograde SE or SBE. Patient demographics, indication for procedure, DMI, procedure time, therapeutic procedure time, adverse event, diagnostic findings, and therapeutic interventions were prospectively recorded. The primary outcome was DMI. Secondary outcomes included: procedure time; diagnostic yield; therapeutic yield and adverse event rates.</p><p><strong>Results: </strong>During the study period, 30 patients underwent deep enteroscopy (SE 13, SBE 17). The most common indication was gastrointestinal bleeding in both groups. There was no significant difference in the DMI between SE and SBE (330.0 ± 88.2 cm vs 285.3 ± 80.8 cm, <i>P</i> = .16). There was no difference between SE and SBE in procedure time (37.0 ± 10.5 vs 38.3 ± 12.4, <i>P</i> = .76), diagnostic yield (SE = 9 [69%] vs SBE = 7 [41%], <i>P</i> = .16), or therapeutic yield (SE = 6 [46%] vs SBE = 4 [24%], <i>P</i> = .26). There were no major adverse events in either group.</p><p><strong>Conclusions: </strong>Spiral enteroscopy and SBE are similar with respect to DMI, diagnostic yield, therapeutic yield, procedure time, and rate of adverse events. Small numbers prevent giving a definitive judgment and future adequately powered prospective study is required to confirm these findings.</p>\",\"PeriodicalId\":10382,\"journal\":{\"name\":\"Clinical Medicine Insights. Gastroenterology\",\"volume\":\" \",\"pages\":\"1179552218754881\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-01-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/aa/10.1177_1179552218754881.PMC5788085.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179552218754881\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179552218754881","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A Randomized Controlled Trial Comparing the Depth of Maximal Insertion Between Anterograde Single-Balloon Versus Spiral Enteroscopy.
Background: Three device-assisted deep endoscopic platforms presently exist and are available for clinical use: double-balloon enteroscopy, single-balloon enteroscopy (SBE), and spiral enteroscopy (SE). In a retrospective study, SE was associated with a greater depth of maximal insertion (DMI) with similar diagnostic yields and procedure time as compared with SBE.
Aims: This was a prospective, randomized comparison of SE and SBE with respect to DMI, diagnostic yield, procedure time, and rate of adverse events.
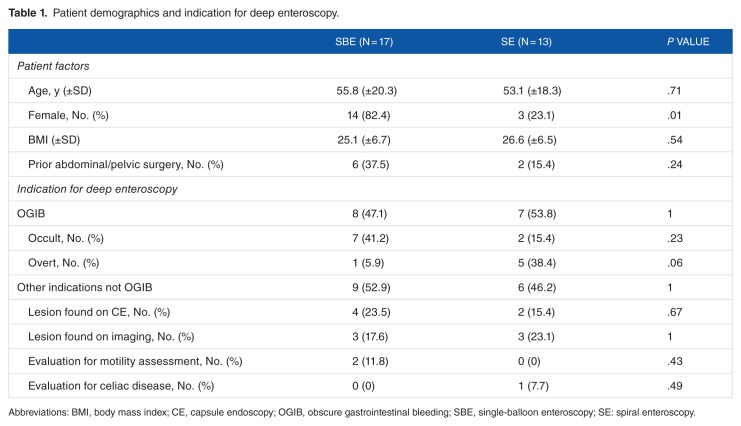
Methods: Patients were prospectively randomized to undergo either anterograde SE or SBE. Patient demographics, indication for procedure, DMI, procedure time, therapeutic procedure time, adverse event, diagnostic findings, and therapeutic interventions were prospectively recorded. The primary outcome was DMI. Secondary outcomes included: procedure time; diagnostic yield; therapeutic yield and adverse event rates.
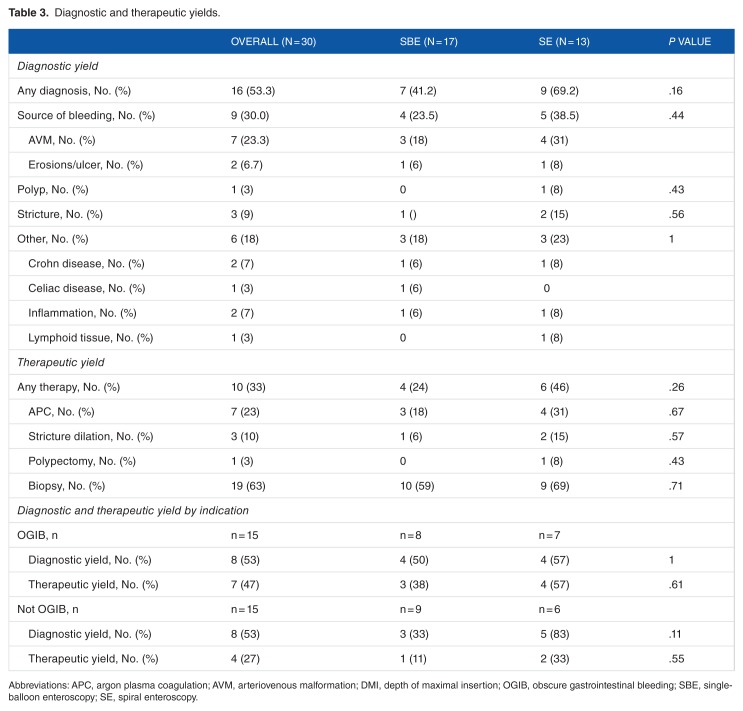
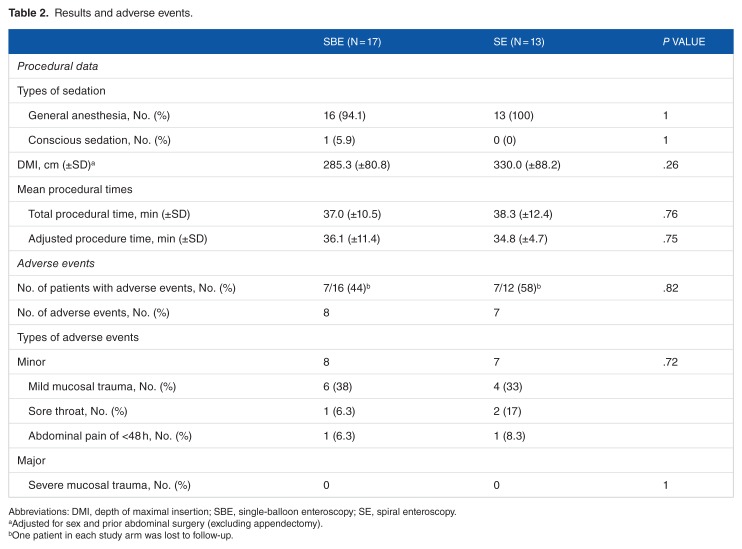
Results: During the study period, 30 patients underwent deep enteroscopy (SE 13, SBE 17). The most common indication was gastrointestinal bleeding in both groups. There was no significant difference in the DMI between SE and SBE (330.0 ± 88.2 cm vs 285.3 ± 80.8 cm, P = .16). There was no difference between SE and SBE in procedure time (37.0 ± 10.5 vs 38.3 ± 12.4, P = .76), diagnostic yield (SE = 9 [69%] vs SBE = 7 [41%], P = .16), or therapeutic yield (SE = 6 [46%] vs SBE = 4 [24%], P = .26). There were no major adverse events in either group.
Conclusions: Spiral enteroscopy and SBE are similar with respect to DMI, diagnostic yield, therapeutic yield, procedure time, and rate of adverse events. Small numbers prevent giving a definitive judgment and future adequately powered prospective study is required to confirm these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


